History of Present Illness
17-year-old male presents 10 days post-tonsillectomy (performed at St. Michael's for recurrent strep throat) with an episode of spitting up a 'couple mouthfuls' of blood starting about an hour prior to arrival. Patient denies any other medical problems, takes no medications, and specifically denies aspirin use. Lungs are clear bilaterally with no stridor. No abdominal pain or nausea initially. Parents are currently out of town.

Emergency Department Course
Triage & Initial Evaluation
Patient arrival with post-op hemoptysis.
+1
Triage & Initial Evaluation
Patient arrival with post-op hemoptysis.
Medical Decision Making
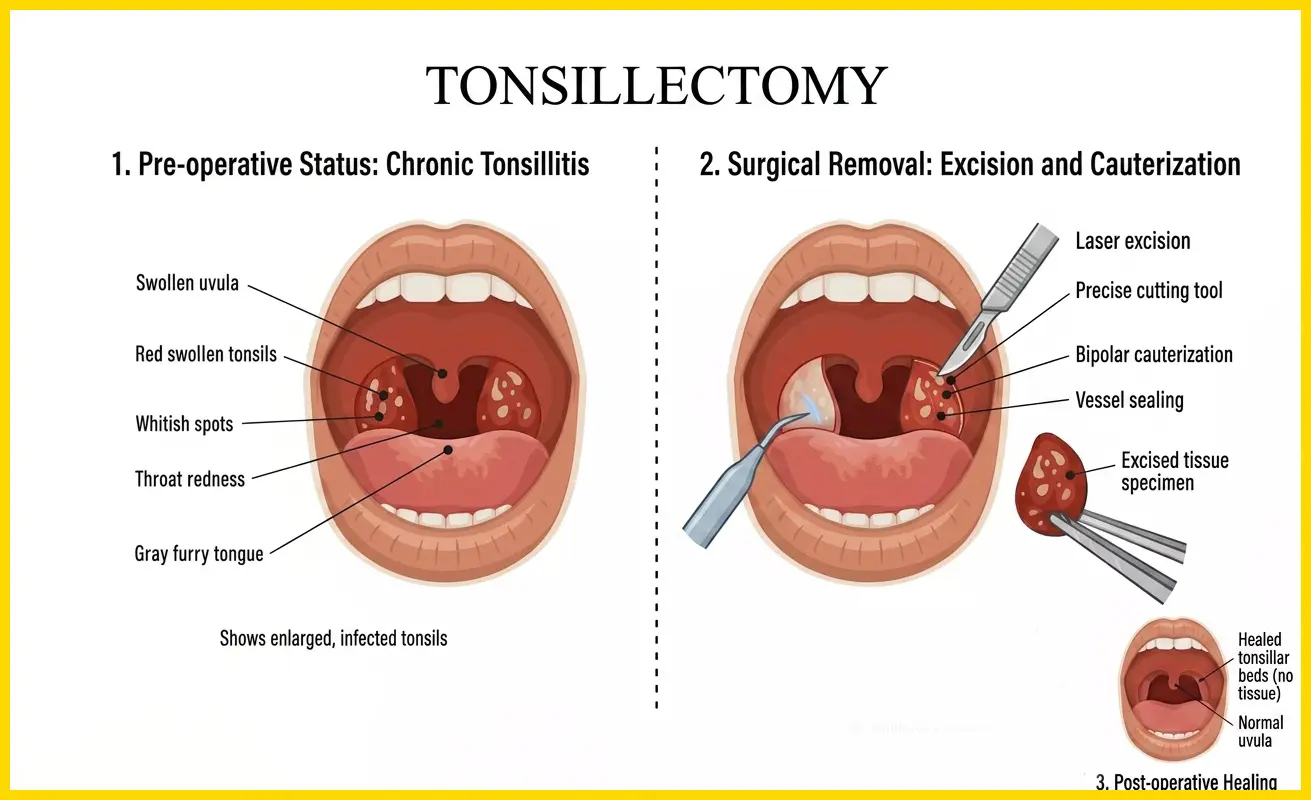
Post-tonsillectomy hemorrhage (PTH) can be divided into primary (<24 hours) and secondary (>24 hours, typically 5-10 days post-op as the eschar sloughs off). Even minor bleeding (herald bleeds) requires aggressive evaluation because it can rapidly progress to massive hemorrhage. The immediate goal is to stabilize the clot, reverse any coagulopathy, and get definitive surgical backup (ENT) to bedside.
Diagnostics & Findings
- CBC
- BMP
- Coagulation panel
- Type and Screen
Findings:
- No active bleeding visualized
- Fibrinous clot (white/dark brown eschar) noted in tonsillar fossae
Interventions
- Nebulized Tranexamic Acid (TXA)
⮑ Outcome & Reassessment
Bleeding has temporarily ceased; fibrinous clot is stable. Patient is instructed to take slow, deep breaths with the nebulizer. Whitaker is left to monitor the patient and contact Head and Neck.
Clinical Media
Clinical Deterioration & Massive Hemorrhage
Sudden massive oral hemorrhage after the clot dislodges.
+1
Clinical Deterioration & Massive Hemorrhage
Sudden massive oral hemorrhage after the clot dislodges.
Medical Decision Making
The herald bleed has evolved into a massive secondary hemorrhage. The patient is at immediate risk of exsanguination and asphyxiation from blood pooling in the airway. Rapid Sequence Intubation (RSI) is necessary to protect the airway, using Ketamine as a hemodynamically stable induction agent. Direct pressure using a sponge stick is a temporizing measure to stem the bleeding while preparing for airway takeover and resuscitation.
Diagnostics & Findings
Findings:
- Copious active oral bleeding
- Tachycardia (120 bpm)
- Hypoxia (SpO2 90%)
Interventions
- Yankauer suction
- Direct pressure to tonsillar fossa via sponge stick
- Order 2 units Whole Blood
- Place second IV line
- High-flow nasal cannula
- Ketamine 100mg IV for induction
⮑ Outcome & Reassessment
Patient is choking on blood, tachycardic, and hypoxic. Sedation takes effect, leading into a difficult airway scenario.
Clinical Media

Failed Airway / CICO Preparation
Inability to intubate due to massive bleeding obscuring the vocal cords.
Failed Airway / CICO Preparation
Inability to intubate due to massive bleeding obscuring the vocal cords.
Medical Decision Making
This is a classic 'Can't Intubate, Can't Oxygenate' (CICO) scenario secondary to a soiled airway. Suction is inadequate to clear the visual field. A blind attempt with a bougie feeling for tracheal rings is a low-probability salvage technique. Dr. Yolanda Garcia recognizes the imminent need for a definitive surgical airway (cricothyrotomy) to prevent hypoxic arrest.
Diagnostics & Findings
- GlideScope video laryngoscopy (view obscured by blood)
Findings:
- Grade 4 view (nothing but blood)
- Progressive desaturation
Interventions
- Blind intubation attempt via Bougie (Failed)
- Opening cricothyrotomy tray and prepping the neck
⮑ Outcome & Reassessment
SpO2 continues to fall to 87%. The patient is at extreme risk of death. Robby prepares the scalpel for a surgical airway.
Retrograde Intubation
Impending need for cricothyrotomy due to profound hypoxia.
+1
Retrograde Intubation
Impending need for cricothyrotomy due to profound hypoxia.
Medical Decision Making
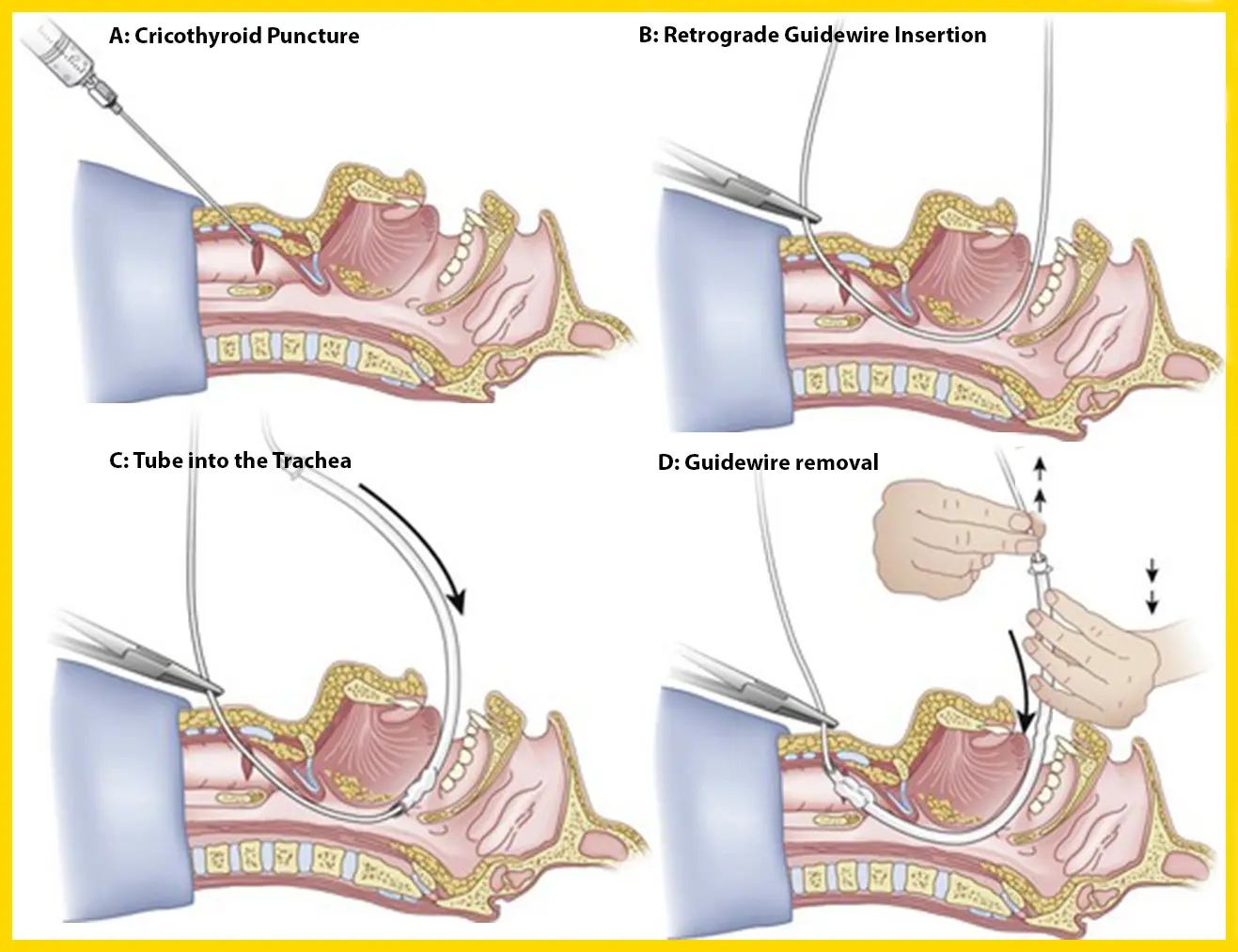
Before making a scalpel incision for a surgical airway, Dr. Robby attempts a retrograde intubation. This involves passing a needle and guidewire through the cricothyroid membrane, angling cephalad (upward), retrieving the wire from the mouth, and railroading the endotracheal tube down over the wire into the trachea. It avoids the morbidity of a full surgical airway while bypassing the visually obscured oropharynx.
Diagnostics & Findings
Findings:
- Wire retrieved from oral cavity
- Tube successfully passed to 25cm at the lips
Interventions
- Bag-valve-mask (BVM) ventilation temporarily
- Retrograde intubation
- Cuff inflation
- End-tidal CO2 confirmed (Yellow)
⮑ Outcome & Reassessment
Successful airway securement. Bilateral breath sounds confirmed. SpO2 rapidly improves to 90%, then 92%. Patient is stabilized.
Clinical Media
Definitive Care & Handoff
Airway secured, patient requires definitive surgical hemostasis.
Definitive Care & Handoff
Airway secured, patient requires definitive surgical hemostasis.
Medical Decision Making
With the airway secured and the bleeding temporarily controlled via direct sponge-stick pressure, the patient must be kept heavily sedated to prevent extubation or dislodgment of the clot. The patient is ready for emergent transport to the Operating Room for definitive vessel ligation/cautery by the ENT surgeon.
Diagnostics & Findings
Findings:
- Bleeding controlled with direct pressure
- Patient stable for transport
Interventions
- Propofol drip initiated
- Fentanyl drip initiated
- Maintenance of direct pressure with fresh sponge stick
- Transport to Operating Room
⮑ Outcome & Reassessment
Patient remains hemodynamically stable post-intubation and is successfully handed off to ENT.
Diagnoses & Disposition
Evolving Diagnoses
- [S01E05]Secondary Post-Tonsillectomy Hemorrhage (Herald Bleed)
- [S01E05]Massive Upper Airway Hemorrhage / Hemorrhagic Shock
- [S01E05]Failed Airway (Can't Intubate, Can't Oxygenate)
Current Disposition
Admitted to the Operating Room under the care of Head and Neck Surgery (ENT) for definitive hemostasis.
Casebook Analysis
Episode Context
Travis serves as a high-stakes, adrenaline-fueled emergency that highlights the unpredictability of seemingly minor post-operative complications. The case creates intense dramatic tension, forces Whitaker to manage an exploding crisis, and allows Dr. Robby to demonstrate exceptional airway skills to save the patient and spare Dr. Garcia from performing a more invasive surgical airway. It also highlights the systemic issue of consulting services (ENT) refusing to see patients who had their original procedures at different hospitals.
Attending's Review
Medical Accuracy
The progression of the case is highly medically accurate. Secondary post-tonsillectomy hemorrhages commonly occur between days 5-10 as the eschar sloughs off. A 'herald bleed' (spitting up a mouthful of blood) is a warning sign that massive, potentially fatal arterial bleeding is imminent. The initial management with nebulized TXA is a modern, evidence-based temporizing measure. The depiction of a soiled airway causing a CICO (Can't Intubate, Can't Oxygenate) scenario is realistic and terrifying. While retrograde intubation is a real technique, it is exceedingly rare in modern EDs, which usually rely on SALAD (Suction Assisted Laryngoscopy and Airway Decontamination) or move straight to a scalpel-finger-bougie cricothyrotomy.
Complications & Errors
- Retrograde Intubation vs. SALAD: While Dr. Robby successfully utilized retrograde intubation, modern Emergency Medicine algorithms heavily favor the SALAD (Suction Assisted Laryngoscopy and Airway Decontamination) technique for massively soiled airways. SALAD uses continuous, large-bore rigid suction (often pinned into the esophagus) to clear the visual field for standard laryngoscopy. Because retrograde intubation is time-consuming and technically complex, it has largely fallen out of favor for crashing, desaturating patients. In a real-world scenario, if SALAD fails to secure an actively bleeding airway, providers typically move directly to a scalpel-finger-bougie surgical cricothyrotomy rather than attempting a retrograde wire passage.
Clinical Pearls
Herald bleed: a minor, early episode of bleeding that serves as a warning sign of an impending, massive arterial hemorrhage. In post-tonsillectomy patients, this typically occurs 5-10 days post-op as the protective fibrinous eschar sloughs off, exposing fragile underlying blood vessels. Dr. Robby correctly recognized that the patient's seemingly mild hemoptysis (a couple mouthfuls) indicated an unstable eschar, which is why he was prepared for the situation to 'go south pretty quickly' before the actual massive hemorrhage occurred.
Never discharge a 'herald bleed' post-tonsillectomy. Even if the bleeding has stopped upon ED arrival, these patients must be evaluated by ENT, as the clot can dislodge resulting in massive arterial hemorrhage.
Nebulized Tranexamic Acid (TXA) is an excellent, non-invasive temporizing adjunct for oral and pharyngeal bleeding while definitive care is mobilized.
In massive upper GI/ENT bleeds, be prepared for a difficult airway. Have dual large-bore suction (Duanto/Yankauer), prepare for the SALAD technique, and have your surgical airway kit open and ready before pushing induction drugs.
Retrograde intubation is a rare but vital salvage airway technique for cases where the vocal cords cannot be visualized from above, such as a massively soiled airway (e.g., hemorrhage, emesis) or severe anatomical distortion. By passing a guidewire upward through the cricothyroid membrane and retrieving it from the mouth, clinicians can railroad the endotracheal tube directly into the trachea, securing the airway while avoiding the morbidity of a front-of-neck surgical cricothyrotomy.