History of Present Illness
53-year-old male presents with a leg wound sustained 10 days ago during a mountain biking trip in Moab, Utah, after jamming a pedal into his leg. He has been applying topical Neosporin, but reports the pain has progressively worsened and it now hurts to walk. Initial examination shows road rash with surrounding cellulitis and a central blood blister/hematoma.

Emergency Department Course
Initial Assessment & Triage
Patient placed in ED bay for evaluation of infected leg wound.
+1
Initial Assessment & Triage
Patient placed in ED bay for evaluation of infected leg wound.
Medical Decision Making
Wound appears to have developed secondary bacterial infection (cellulitis) around the primary site of impact. The central area contains a blood blister (hematoma) that requires debridement to remove devitalized tissue and promote proper healing.
Diagnostics & Findings
- Physical examination of the wound
Findings:
- Erythematous border consistent with cellulitis
- Central simple hematoma / blood blister covered by devitalized skin
Interventions
- Prescribed oral antibiotics
- Planned mechanical debridement of dead skin over the blister
⮑ Outcome & Reassessment
Patient is agreeable to the plan and understands the need for debridement. Student doctor Whitaker is tasked with setting up the sterile field (Iris scissors, toothed forceps, sterile gauze...) and performing the debridement.
Clinical Media

Procedural Complication & Hemorrhage Control
Sudden, massive arterial bleeding during routine wound debridement.
+2
Procedural Complication & Hemorrhage Control
Sudden, massive arterial bleeding during routine wound debridement.
Medical Decision Making
The 'simple hematoma' was actually a ballotable vesicle covering a lacerated arteriole. Puncturing the roof of the blister removed the tamponade effect, resulting in immediate arterial hemorrhage. Immediate mechanical hemostasis is required before definitive repair.
Diagnostics & Findings
- Visual identification of pulsatile arterial bleeding
Findings:
- Arterial pumper identified beneath the previously intact blood blister
Interventions
- Applied blood pressure cuff proximal to the wound
- Inflated BP cuff to 180 mmHg to serve as a makeshift tourniquet
- Injected 10 ccs of 1% lidocaine with epinephrine to achieve local anesthesia and induce localized vasoconstriction
⮑ Outcome & Reassessment
Bleeding successfully halted by the BP cuff tourniquet. Patient experienced sudden pain and panic, but was calmed once the bleeding was controlled.
Clinical Media


Vascular Repair
Need for definitive ligation of the bleeding arteriole so the tourniquet can be safely removed.
+1
Vascular Repair
Need for definitive ligation of the bleeding arteriole so the tourniquet can be safely removed.
Medical Decision Making
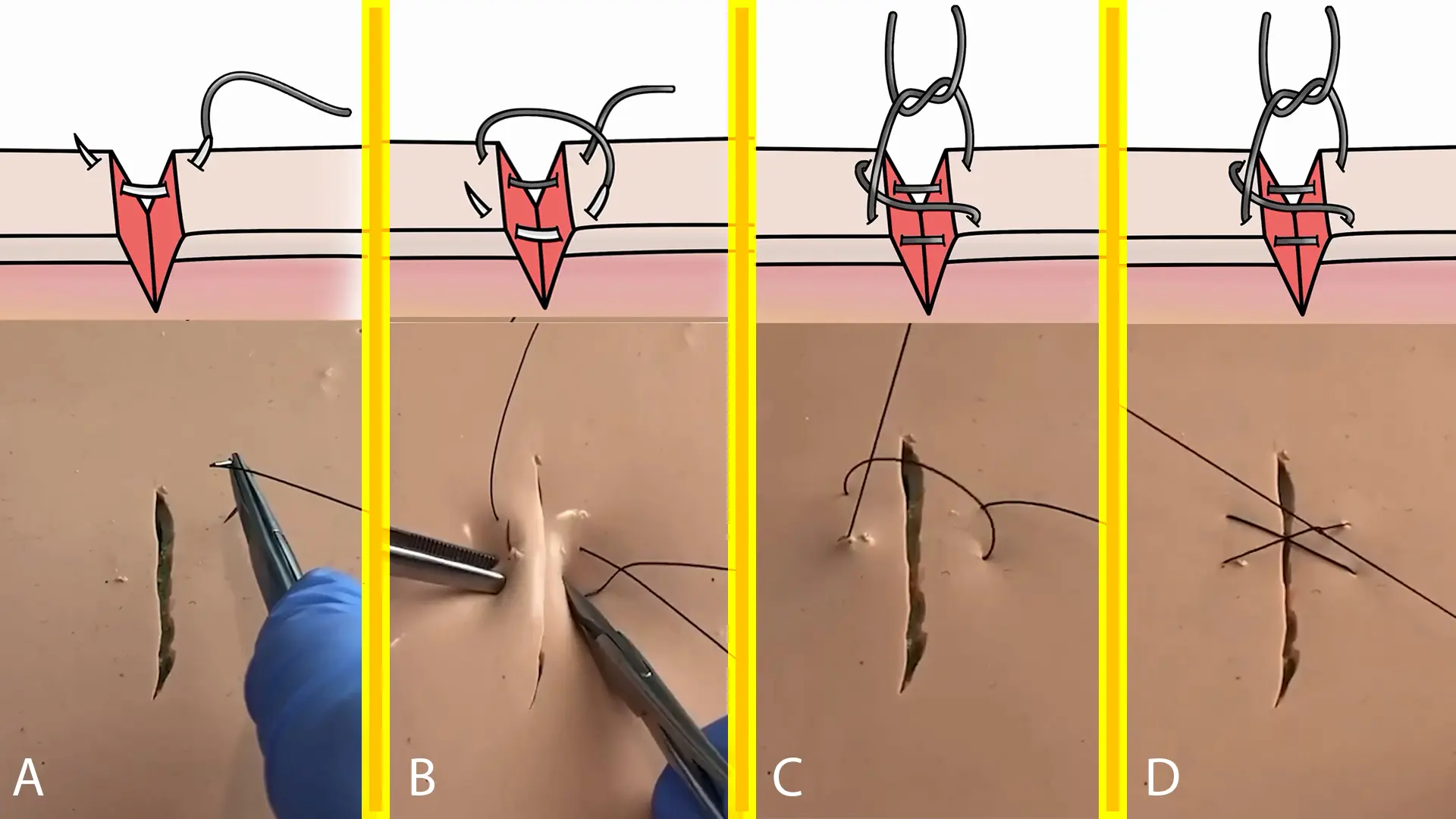
By slowly deflating the BP cuff, the exact pinpoint location of the arteriole can be identified. A figure-of-eight suture is optimal here as it grabs a broad bite of tissue to secure the vessel effectively, providing reliable hemostasis for small, retracted, or difficult-to-isolate bleeders.
Diagnostics & Findings
- Controlled deflation of the BP cuff to visualize the bleeding source
Findings:
- Exact site of the severed arteriole visualized within the wound bed
Interventions
- Set up suture tray with 3-0 nylon
- Placed a figure-of-eight suture (a simple interrupted suture anterior to the bleeder, followed by a posterior bite before tying)
⮑ Outcome & Reassessment
Hemostasis achieved successfully. The complication was framed as a life-saving 'catch', noting that if the blister had eroded at home without medical intervention, the patient could have experienced uncontrollable hemorrhage.
Clinical Media
Diagnoses & Disposition
Evolving Diagnoses
- [S01E05]Cellulitis of the lower extremity with overlying simple hematoma
- [S01E05]Concealed arterial laceration beneath a ballotable vesicle
Current Disposition
Wound successfully debrided and arteriole ligated. Pending discharge with oral antibiotics.
Casebook Analysis
Episode Context
The case serves as a character-building moment for the medical student Dennis Whitaker (MS4). Frustrated by being assigned to what he perceives as a boring blister guy, Later, Dr. Mohan frames the event as a life-saving catch, teaching Whitaker that even seemingly minor complaints can mask severe complications, boosting his confidence.
Attending's Review
Medical Accuracy
The presentation is highly realistic. Traumatic hematomas can occasionally mask deeper vascular injuries or form pseudoaneurysms. Puncturing them releases the tamponade effect, leading to immediate arterial bleeding. Mel's response of throwing a blood pressure cuff on the limb and inflating it above systolic pressure (180 mmHg) is a textbook, rapid, and highly effective ED maneuver for extremity bleeding. The choice of 1% lidocaine with epinephrine is correct to assist with vasoconstriction, and the figure-of-eight suture is standard for this type of hemostasis.
Complications & Errors
- Whitaker failed to palpate the blister for pulsatility (ballotable vesicle) prior to incising it. Blindly debriding an unassessed hematoma over a trauma site risks exactly the type of arterial hemorrhage seen here.
Clinical Pearls
Always palpate post-traumatic hematomas for pulsatility to rule out pseudoaneurysms or underlying arterial injury before performing an incision and drainage or debridement.
Arterial bleeding presents as bright red, high-pressure, pulsatile jets (synchronous with the heartbeat), whereas venous bleeding is typically dark red with a steady, lower-pressure flow. Arterial bleeds require immediate high-pressure control (e.g., proximal tourniquets, pinpoint direct pressure, or surgical ligation), whereas venous bleeds can often be managed with direct wound pressure and elevation.
A standard blood pressure cuff inflated above systolic pressure is an excellent, readily available tourniquet to achieve temporary hemostasis in the ED.
The Figure-of-Eight Suture Mechanics: This technique acts as essentially two simple interrupted sutures combined into one continuous stitch. Its primary benefit is providing broad tissue compression over a larger surface area. In cases like this, where a severed arteriole retracts into the surrounding tissue and is difficult to isolate directly, a figure-of-eight suture securely transfixes the vessel and adjacent tissue bed to reliably halt the hemorrhage.
A figure-of-eight suture is highly effective for securing hemostasis in a bleeding vessel, especially when the vessel is retracted or pinpoint ligation is difficult.


