History of Present Illness
Kristi Wheeler is a 17-year-old female (G1P0) presenting to the ED with her mother, Lynette, for a scheduled medication abortion. They initially had an appointment with Dr. Abbot at 06:30 but overslept and arrived hours later. The patient's last menstrual period (LMP) was approximately the 23rd of June. She denies any known drug allergies and has no prior surgical history.

Emergency Department Course
Initial Provider Assessment & Pre-Procedure Evaluation
Patient evaluation prior to administering abortifacients.
+1
Initial Provider Assessment & Pre-Procedure Evaluation
Patient evaluation prior to administering abortifacients.
Medical Decision Making
Dr. Collins is taking over care from the off-going Dr. Abbot. Before administering a medication abortion (typically mifepristone followed by misoprostol), Dr. Collins must establish the patient's medical history, assess gestational age via LMP, and verify there are no medical or surgical contraindications. Most critically, an ultrasound must be ordered to confirm an intrauterine pregnancy, date the gestation to ensure it falls within the safe therapeutic window (typically < 70 days), and rule out an ectopic pregnancy.
Diagnostics & Findings
- Clinical history intake
- Pelvic ultrasound
Findings:
- First pregnancy (G1P0)
- LMP: June 23 (approximate)
- No drug allergies
- No prior surgical history
Interventions
- Instructed patient to change into a hospital gown for the pending ultrasound examination.
⮑ Outcome & Reassessment
Patient is cooperative, denies any allergies or past medical issues, and prepares for the ultrasound.
Clinical Media

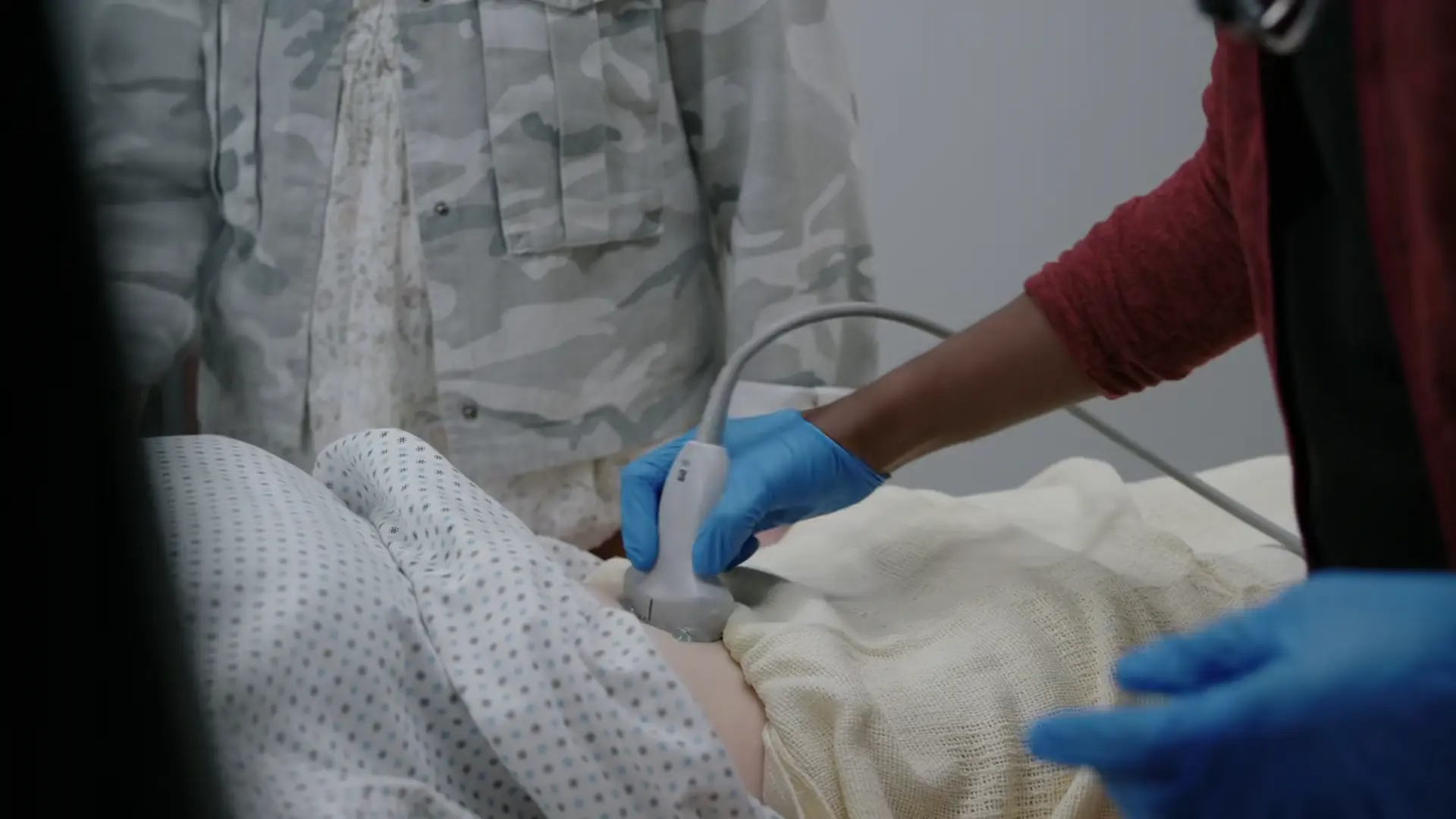
Diagnostic Imaging (Ultrasound)
Routine pre-medication abortion ultrasound to confirm gestational age.
+2
Diagnostic Imaging (Ultrasound)
Routine pre-medication abortion ultrasound to confirm gestational age.
Medical Decision Making
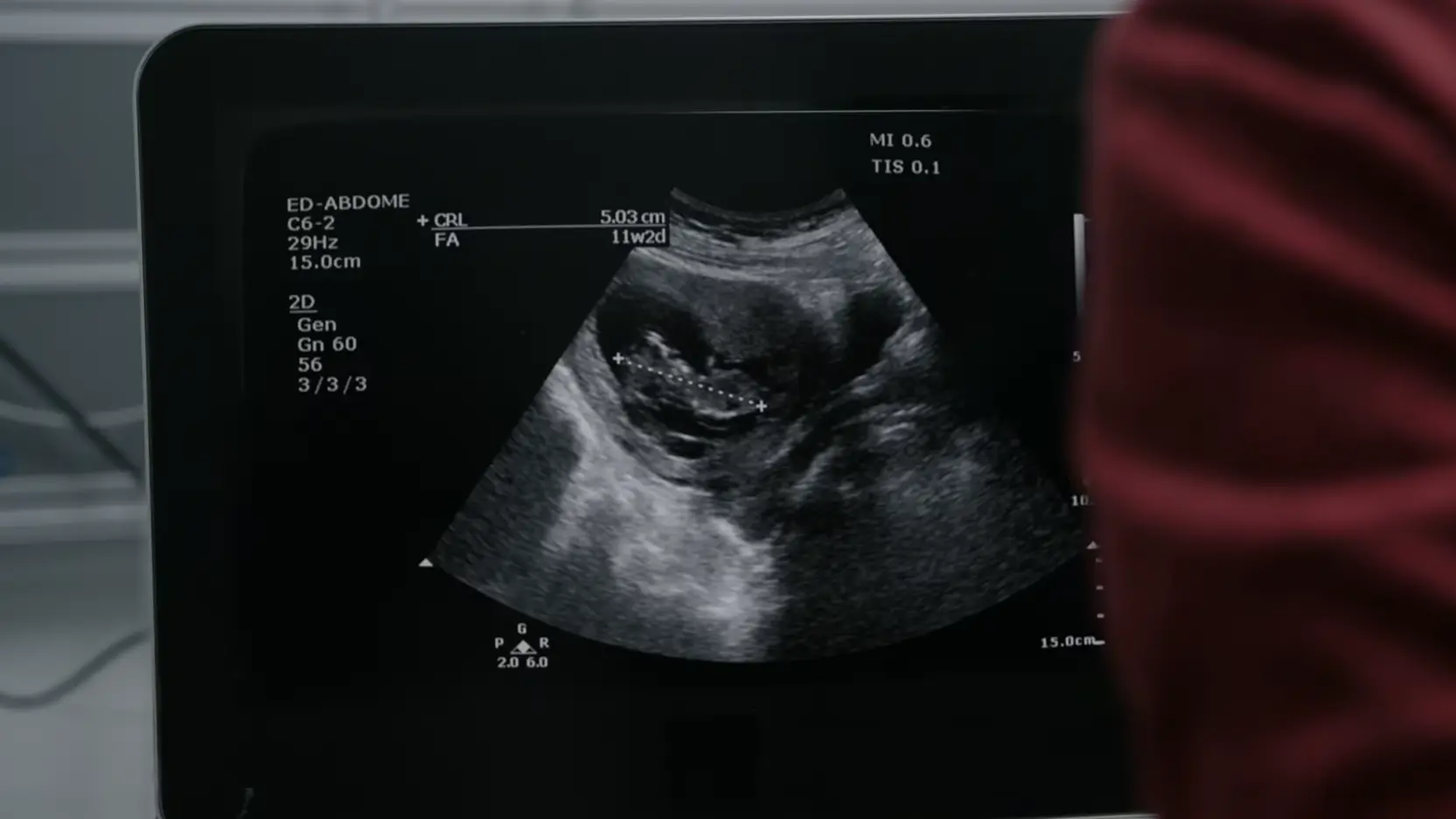
Dr. Collins performs an ultrasound and measures the Crown-Rump Length (CRL) at 5.03 cm, which correlates to an Estimated Gestational Age (EGA) of 11 weeks and 2 days. This is a critical inflection point: it means the patient's pregnancy is further along than her LMP suggested. At 11w2d, the patient exceeds the standard FDA-approved 70-day (10-week) limit for outpatient mifepristone/misoprostol regimens. Given the current complex legal landscape around abortion access, Dr. Collins recognizes this finding may cross a strict gestational cutoff, prompting her to recalculate the measurements to be absolutely certain.
Diagnostics & Findings
- Transabdominal Pelvic Ultrasound
Findings:
- Intrauterine pregnancy confirmed.
- CRL: 5.03 cm
- Estimated Gestational Age: 11 weeks, 2 days.
Interventions
- Ultrasound imaging captured; measurements recalculated to ensure diagnostic accuracy.
⮑ Outcome & Reassessment
Patient senses the provider's hesitation and asks 'Is everything okay?'. Dr. Collins replies 'Yeah' to maintain composure while internally processing the complication.
Clinical Media
Ethical Conflict
Discovery of gestational age exceeding the 11-week medication abortion cutoff.
Ethical Conflict
Discovery of gestational age exceeding the 11-week medication abortion cutoff.
Medical Decision Making
Dr. Collins compares her ultrasound measurements (Gestational Sac: 11w3d, Biparietal Diameter: 11w1d) to Dr. Abbot's previous measurements (10w5d) and determines the patient is objectively past the mandated 11-week cutoff for a medication abortion. Recognizing the ethical and legal risks, Dr. Collins refuses to falsify the chart. Dr. Robinavitch, acting as the attending, decides to take over the case, erase Dr. Collins' H&P, and perform a new ultrasound to deliberately capture an image demonstrating a gestational age under 11 weeks, prioritizing the 17-year-old's desire for the procedure over strict legal/ethical compliance.
Diagnostics & Findings
- Review of previous ultrasound measurements (Abbot vs. Collins)
Findings:
- Collins' measurements: Gestational sac 11w3d, BPD 11w1d, consistent with >11 weeks.
- Abbot's measurements: 10w5d.
Interventions
- Dr. Robinavitch assumes primary care of the patient.
- Decision made to overwrite the medical record with a new, intentionally manipulated ultrasound measurement.
⮑ Outcome & Reassessment
N/A - patient not present for this discussion.
Diagnostic Ultrasound
Need to document a gestational age under 11 weeks to proceed with medication abortion.
Diagnostic Ultrasound
Need to document a gestational age under 11 weeks to proceed with medication abortion.
Medical Decision Making
Dr. Robinavitch performs a repeat ultrasound. He measures the Crown-Rump Length (CRL) selectively to obtain a result of 10 weeks and 6 days. This measurement places the patient just under the 11-week hospital/state cutoff, allowing him to legally order the Mifepristone and Misoprostol, circumventing earlier measurements.
Diagnostics & Findings
- Transabdominal Pelvic Ultrasound
Findings:
- Documented CRL correlating to 10 weeks, 6 days.
Interventions
- Prescribed Mifepristone and Misoprostol regimen.
⮑ Outcome & Reassessment
Patient is relieved she made the cutoff by one day.
Consent Revocation
Dispensing abortifacients and providing patient education.
+1
Consent Revocation
Dispensing abortifacients and providing patient education.
Medical Decision Making
Dr. Collins is providing discharge instructions for a >10-week medication abortion protocol: Mifepristone twice (now and in 24 hours), followed by Misoprostol 24 hours after that (two buccal pills, then two more 6 hours later). She advises returning to the ED if bleeding exceeds two pads an hour or for severe pain. The process is abruptly halted when the patient's actual biological mother arrives, revealing that the accompanying adult is the patient's aunt. Because the patient is a minor, the biological mother revokes consent, legally barring the administration of the abortion medication.
Diagnostics & Findings
- Verification of parental consent (failed)
Findings:
- Accompanying adult identified as aunt, not legal guardian.
- Biological mother revokes medical consent for the minor.
Interventions
- Medication abortion halted.
- Instructions provided but medication not administered.
⮑ Outcome & Reassessment
Patient's mother refuses the procedure ('Not now, not ever'). Abortion is canceled.
Clinical Media
Diagnoses & Disposition
Evolving Diagnoses
- [S01E04]First Trimester Pregnancy (Pending Ultrasound Confirmation)
- [S01E04]Intrauterine Pregnancy - 11 weeks, 2 days
- [S01E05]Intrauterine Pregnancy - 10 weeks, 6 days
- [S01E05]Medication abortion canceled (Lack of parental consent)
Current Disposition
Medication abortion canceled due to revocation of parental consent by the patient's biological mother; patient remains in the ED with family.
Casebook Analysis
Episode Context
Kristi and her mother arrive for a medication abortion but missed their original time slot with Dr. Abbot because they overslept and failed to set an alarm. Dr. Heather Collins steps in to assume care. However, during the routine ultrasound, Dr. Collins discovers the fetus is at 11 weeks and 2 days exceeding typical medication abortion limits. This introduces a significant legal and procedural conflict, raising the stakes of their initial tardiness. In S01E05, the gestational age discrepancy causes a conflict between Dr. Collins and Dr. Robinavitch. Dr. Collins refuses to falsify records, so Dr. Robinavitch takes over, manipulating a new ultrasound to measure 10w6d, just under the 11-week cutoff. Dr. Collins prepares to administer the medication, but the procedure is halted when Kristi's biological mother arrives. It is revealed the adult accompanying Kristi was her aunt, and the mother legally revokes consent for the minor's abortion.
Attending's Review
Medical Accuracy
The protocol demonstrated by Dr. Collins is highly accurate for a clinical or ED setting handling early pregnancy terminations. Before dispensing mifepristone and misoprostol, it is the standard of care to obtain the Last Menstrual Period (LMP), confirm the patient's allergy profile, check surgical history, and perform an ultrasound. The ultrasound is a critical safety measure to confirm the pregnancy is intrauterine (ruling out life-threatening ectopic pregnancy) and to verify gestational dating. The FDA approves mifepristone for use up to 70 days (10 weeks) gestation. Finding a CRL of 5.03 cm correctly correlates to an 11w2d gestation, accurately triggering a clinical pivot and validating the provider's need to double-check her measurements. In S01E05, the show introduces an '11-week cutoff' for medication abortion. While FDA labeling is up to 10 weeks (70 days), the WHO and some off-label evidence-based protocols allow medication abortion up to 11 or 12 weeks with modified dosing (e.g., additional misoprostol). The show's >10-week regimen (mifepristone twice, then misoprostol buccal doses) reflects an intensive off-label approach. Ethically, Dr. Robinavitch's decision to delete a colleague's chart and falsify ultrasound measurements is a severe HIPAA violation, constitutes medical fraud, and could result in loss of licensure. Additionally, failing to verify legal guardianship of a minor before an elective procedure is a massive medicolegal liability.
Complications & Errors
- Patient non-compliance/delay (missed original 06:30 appointment), which resulted in prolonged wait times and a provider handoff.
- Dr. Robinavitch deliberately manipulated an ultrasound angle and falsified medical records to document a gestational age (10w6d) under the 11-week cutoff, which is illegal and unethical.
- The initial intake failed to properly verify the identity and legal guardianship of the accompanying adult, leading to an aborted procedure when the biological mother arrived and revoked consent.
Clinical Pearls
Pennsylvania Abortion Law & The 11-Week Medication Cutoff: In Pennsylvania, abortion is legally permitted up to 23 weeks and 6 days. The strict '11-week cutoff' referenced in the episode is not a state-wide ban on abortion, but rather a clinical and institutional limit specifically for medication abortion (mifepristone/misoprostol). While FDA labeling approves the regimen up to 10 weeks, many PA clinics utilize evidence-based off-label protocols up to exactly 11 weeks (77 days). For a pregnancy at 11w2d, standard practice in PA requires pivoting to an in-clinic procedural (surgical) abortion. Additionally, PA state law mandates parental consent (or a judicial bypass) and a 24-hour waiting period for minors.
Always obtain a baseline pelvic ultrasound prior to prescribing mifepristone and misoprostol to confirm an intrauterine pregnancy and definitively rule out ectopic pregnancy. Always rely on ultrasound Crown-Rump Length (CRL) for definitive dating in the first trimester, as patient-reported LMP is frequently inaccurate.
Mechanism of Action: Mifepristone is a competitive progesterone receptor antagonist that causes decidual necrosis, cervical softening, and sensitizes the myometrium. Misoprostol, administered 24-48 hours later, is a synthetic prostaglandin E1 (PGE1) analog that induces strong uterine contractions and cervical ripening to expel the pregnancy.
The US Legal Landscape & Local Disparities: Following the 2022 Dobbs decision overturning Roe v. Wade, abortion access in the US is highly fragmented, ranging from total state bans to protected access. In Pittsburgh, Pennsylvania, abortion remains legally protected up to 23 weeks and 6 days. However, because the FDA-approved limit for outpatient medication abortion is 10 weeks (70 days), an 11w2d pregnancy necessitates a clinical shift to a procedural abortion (e.g., suction aspiration) highlighting the complex intersection where state law permits the procedure, but pharmacological guidelines restrict the method.
Gestational Age-Based Medication Abortion Protocols: For pregnancies ≤ 10 weeks (70 days), the standard FDA-approved regimen is a single 200 mg dose of oral mifepristone followed 24–48 hours later by a single 800 mcg dose of buccal or vaginal misoprostol. As the gestational age advances beyond 10 weeks (such as Kristi's situation), more aggressive regimens are required to achieve complete uterine evacuation. The episode depicts this shift by ordering a modified protocol involving repeat doses ('mifepristone twice', and misoprostol repeated 6 hours later). In real-world evidence-based practice (such as WHO guidelines for 10-12 weeks), the mifepristone dose typically remains a single 200 mg administration, but the misoprostol is intensified through repeated dosing (e.g., 800 mcg followed by 400 mcg every 3 hours) to safely and effectively expel the advanced pregnancy.
Patient Counseling and Administration of Abortifacient Pills: The episode accurately depicts standard patient counseling for medication abortion. Misoprostol is often administered buccally ('dissolve between the cheek and the gum') or vaginally to optimize absorption and reduce gastrointestinal side effects compared to oral ingestion. Expected effects include significant uterine cramping and bleeding (often heavier than a normal period, with clots). Providers must clearly communicate red flag warnings for hemorrhage: patients are instructed to return to the ED if they bleed through more than two thick maxi pads per hour for two consecutive hours, experience severe pain unresponsive to NSAIDs, or develop a fever > 100.4°F (38°C) lasting more than 24 hours after misoprostol administration.
Minor Consent Laws: Medical treatment of a minor, especially for elective procedures like abortion, requires strict adherence to state-specific parental consent or notification laws, unless a judicial bypass is obtained. Failure to verify the identity of the consenting adult is a critical medico-legal error.