History of Present Illness
Mr. Ed Gellin is a 52-year-old male with a significant past medical history of hypertension and hyperlipidemia. He arrived via EMS presenting with 20 minutes of acute onset, 10/10 substernal chest pain accompanied by dyspnea and profound diaphoresis. Field EKG flagged a Code STEMI.

Emergency Department Course
Pre-Arrival Notification
EMS radios in a Code STEMI with an ETA of 5 minutes.
Pre-Arrival Notification
EMS radios in a Code STEMI with an ETA of 5 minutes.
Medical Decision Making
Must mobilize the Cath Lab and prepare an open trauma bay to intercept the patient, confirm the EKG, administer medical management, and achieve a fast door-to-balloon time.
Diagnostics & Findings
Interventions
- Reserved Trauma 2 for patient reception
⮑ Outcome & Reassessment
System primed for patient arrival.
Initial Evaluation and Treatment
Patient arrival and handover from EMS.
+2
Initial Evaluation and Treatment
Patient arrival and handover from EMS.
Medical Decision Making
Patient is experiencing an active massive anterior myocardial infarction. The EKG shows 'tombstone' ST elevations, indicating a complete proximal occlusion of the Left Anterior Descending (LAD) artery. Goal is to stabilize, initiate dual antiplatelet/vasodilator therapy, and immediately transport to the Cardiac Cath Lab for percutaneous coronary intervention (PCI).
Diagnostics & Findings
- 12-Lead EKG
- Blood draw
Findings:
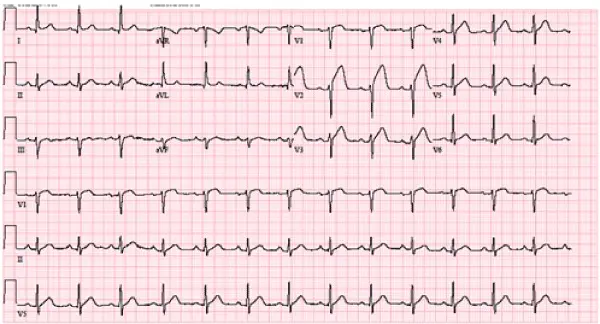
- 7 millimeters ST elevation in the anterior leads ('tombstones')
Interventions
- Chewed 324 mg of baby aspirin
- Second IV line established
- 1 Nitro spray sublingual
- Shaving of insertion site for Cath Lab prep
⮑ Outcome & Reassessment
Patient remains alert, uses humor as a coping mechanism (jokes about a Brazilian wax). Rapidly transferred up to the Cath Lab to hit the 51-minute door-to-balloon target.
Clinical Media
Diagnoses & Disposition
Evolving Diagnoses
- [S01E03]Acute Anterior ST-Elevation Myocardial Infarction (STEMI)
Current Disposition
Transferred to Cardiac Cath Lab for emergent Percutaneous Coronary Intervention (PCI).
Casebook Analysis
Episode Context
Ed Gellin is used to demonstrate a seamless, high-acuity success story for the team. It highlights the ED's capability when protocol is perfectly executed.
Attending's Review
Medical Accuracy
The case is highly accurate to modern emergency medicine protocols. Chewing 324 mg of non-enteric coated aspirin is standard for immediate platelet inhibition. Giving sublingual nitroglycerin for chest pain in the setting of elevated BP (152/95) is appropriate. Emphasizing a 'door-to-balloon' time (target <90 mins standard; they internally push for 51 mins) and recognizing 'tombstone' anterior ST elevations are textbook concepts.
Clinical Pearls
Time is Myocardium: The national benchmark for door-to-balloon time for STEMI patients presenting to a PCI-capable hospital is under 90 minutes. Faster times correlate directly with improved myocardial salvage and reduced mortality.
First-Line Pharmacotherapy (Aspirin & Nitroglycerin): Patients with suspected ACS must CHEW 324 mg of non-enteric coated aspirin. Chewing facilitates rapid buccal and gastric absorption, achieving therapeutic antiplatelet levels much faster than swallowing a pill whole. Concurrently, sublingual nitroglycerin is given for coronary vasodilation and symptom relief, but clinicians must first verify adequate blood pressure (like this patient's 152/95) and rule out right ventricular involvement (highly preload-dependent) or recent PDE-5 inhibitor use to avoid catastrophic hypotension.
Tombstone ST Elevations: Pronounced, convex-upward ST segment elevations that merge with the T wave (resembling a tombstone) in the anterior leads (V1-V4) denote a massive occlusion, usually of the proximal LAD ('Widowmaker').
Aspirin Administration: Patients with acute coronary syndrome should chew 324 mg (or 325 mg) of baby aspirin immediately upon presentation. Chewing ensures rapid buccal and gastric absorption compared to swallowing whole pills.
Similar Cases from The Show



Chart Navigation
Ed Gellin
C/O10/10 substernal chest pain, dyspnea, and diaphoresis.