History of Present Illness
Hank is a construction worker who arrived via EMS/triage after suffering a penetrating injury to his left chest from a framing nail gun. The injury occurred during a workplace 'melee' (scuffle) with his coworker, Joey, who initially pointed the nail gun at his head as a joke. Hank reports severe pain. Denies daily medications or allergies.

Emergency Department Course
Initial Evaluation & Stabilization
Patient arrival as a Tier 1 Trauma for penetrating chest injury.
+1
Initial Evaluation & Stabilization
Patient arrival as a Tier 1 Trauma for penetrating chest injury.
Medical Decision Making
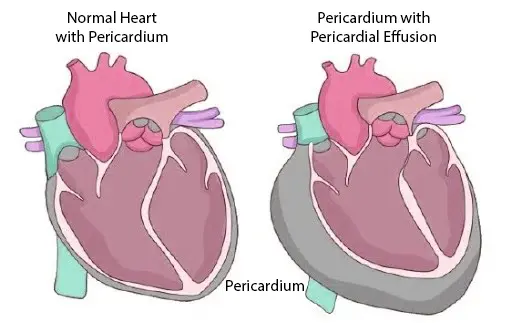
Nail is positioned over the precordium, highly suspicious for intracardiac penetration. The nail is stabilizing the wound and preventing massive hemorrhage; removing it prematurely would be fatal. Tachycardia and borderline blood pressure indicate potential impending decompensation. Need immediate POCUS to check for pericardial effusion/tamponade, pain control, and urgent OR preparation.
Diagnostics & Findings
- Point-of-Care Ultrasound (POCUS) FAST exam
Findings:
- Nail appears intracardiac.
- Small pericardial effusion visualized on ultrasound.
- No evidence of cardiac tamponade at initial scan.
Interventions
- Nail stabilized in place.
- Administered 2mg IV Morphine.
- Prepared 2 units whole blood on standby.
- Consulted OR for immediate cardiac case.
⮑ Outcome & Reassessment
Patient remains highly agitated, demanding the nail be removed and threatening to leave. Maintained borderline hemodynamics long enough to prep for Rapid Sequence Intubation.
Clinical Media
Procedure (Airway Management)
Anticipated hemodynamic collapse and requirement for emergent surgical intervention.
Procedure (Airway Management)
Anticipated hemodynamic collapse and requirement for emergent surgical intervention.
Medical Decision Making
Patient requires emergent transfer to the OR. Given the risk of sudden cardiac tamponade and loss of airway, prophylactic Rapid Sequence Intubation (RSI) is indicated. Ketamine is chosen for induction due to its sympathomimetic profile, preserving what little blood pressure the patient has, paired with succinylcholine for rapid paralysis.
Diagnostics & Findings
Findings:
- Good view of glottis via video laryngoscopy.
Interventions
- Administered 100mg Ketamine and 120mg Succinylcholine.
- Endotracheal intubation performed by Javadi under supervision.
⮑ Outcome & Reassessment
Intubation successful. Airway secured.
Clinical Crash & Surgical Resuscitation
Sudden profound hypotension. Repeat ultrasound shows growing effusion with Right Ventricular (RV) collapse.
+2
Clinical Crash & Surgical Resuscitation
Sudden profound hypotension. Repeat ultrasound shows growing effusion with Right Ventricular (RV) collapse.
Medical Decision Making
Patient has progressed to frank cardiac tamponade. The pericardial sac has filled with blood, exerting pressure that prevents the right ventricle from filling during diastole, causing cardiogenic shock. A needle pericardiocentesis might be considered, but with a penetrating object in situ and rapid collapse, an immediate resuscitative left anterolateral thoracotomy is definitive and required to manually relieve the pressure, remove the object, and repair the myocardium. Selective right mainstem intubation is utilized to intentionally collapse the left lung, keeping it out of the surgical field.
Diagnostics & Findings
- Repeat POCUS
Findings:
- Growing pericardial effusion.
- Right Ventricular (RV) collapse during diastole.
- Single puncture wound identified in the left ventricle.
Interventions
- Advanced ET tube to right mainstem bronchus.
- Initiated massive transfusion (whole blood on infuser).
- Performed Left Anterolateral Thoracotomy.
- Incision made superior to the rib to avoid the neurovascular bundle.
- Placed Finochietto retractor.
- Performed pericardiotomy to release tamponade.
- Extracted the intact framing nail.
- Applied direct digital occlusion to the left ventricular puncture wound.
- Placed a horizontal mattress suture (2-0 Prolene on a tapered needle) for hemostasis.
⮑ Outcome & Reassessment
First unit of blood infused. Blood pressure rapidly improved. The heart filled well with excellent hemostasis achieved at the ventricular repair site. Patient wrapped in moist sterile towels and transferred directly to the OR to meet Cardiothoracic Surgery.
Clinical Media


Diagnoses & Disposition
Evolving Diagnoses
- [S01E03]Penetrating Cardiac Trauma (Left Ventricle)
- [S01E03]Acute Cardiac Tamponade
Current Disposition
Transferred to the Operating Room (Cardiothoracic Surgery) after successful ED resuscitative thoracotomy and stabilization.
Casebook Analysis
Episode Context
Hank's case serves as the episode's high-adrenaline, 'save of the day' trauma arc. It showcases Dr. Garcia's cool-headed competence and aggressive surgical capabilities. It also provides a high-stakes teaching moment for the junior staff member, Dr. Santos.
Attending's Review
Medical Accuracy
The medical depiction is exceptionally accurate. Ketamine is the correct induction agent for a hemodynamically unstable trauma patient. The ultrasound finding of 'Right Ventricular collapse' is the pathophysiologic hallmark of cardiac tamponade. The decision to advance the ET tube into the right mainstem bronchus is a highly realistic, advanced tactical maneuver to intentionally collapse the left lung and gain better surgical exposure during a left thoracotomy. The anatomical teaching point to cut superior to the rib (to avoid the intercostal vein, artery, and nerve) is perfectly correct.
Clinical Pearls
In penetrating chest trauma, never remove the impaled object in the ED until definitive surgical exposure and control are achieved.
The earliest echocardiographic sign of cardiac tamponade is often Right Atrial (RA) systolic collapse, but Right Ventricular (RV) diastolic collapse is highly specific and indicates impending hemodynamic collapse.
When performing a thoracotomy or placing a chest tube, always dissect over the superior margin of the lower rib to avoid the neurovascular bundle (VAN) located along the costal groove at the inferior margin of the rib.
RSI Selection in Trauma: In trauma patients with borderline hemodynamics or suspected cardiac tamponade, Ketamine is the preferred induction agent due to its sympathomimetic properties, which preserve endogenous catecholamine release to maintain heart rate and blood pressure (unlike Propofol, which causes profound hypotension). Pairing it with Succinylcholine provides ultra-rapid onset neuromuscular blockade (30-60 seconds), ensuring the airway is secured safely and swiftly before cardiovascular collapse occurs.
Right mainstem intubation (Advancing the ET tube into the right mainstem bronchus), while usually a complication, can be used intentionally as a poor-man's single-lung ventilation strategy to drop the left lung out of the way during emergency left chest surgeries.
Division of Labor in Resuscitative Thoracotomy: A resuscitative thoracotomy always begins on the left (anterolateral) because it provides the fastest access to the heart and the descending aorta (for cross-clamping). If exposure needs to be widened to address right-sided injuries, the incision is extended across the sternum to create a 'clamshell' thoracotomy. In major trauma centers, roles are clearly delineated to prevent physical crowding: Trauma Surgery takes the primary left side (managing the heart and aorta), while the ED physician takes the right side to manage lung retraction or right thoracic packing.