History of Present Illness
46-year-old female presenting with one hour of right-sided chest pain. Medical history is significant for hyperlipidemia. She received sublingual nitroglycerin and 4mg of morphine in the pre-hospital setting with minimal relief. Initial 12-lead EKG performed by EMS was interpreted as negative for STEMI.

Emergency Department Course
Initial ED Evaluation
Patient arrival via EMS for unresolved chest pain.
+1
Initial ED Evaluation
Patient arrival via EMS for unresolved chest pain.
Medical Decision Making
Patient's presentation is concerning for ACS, but the field EKG is negative for STEMI. With a HEART score of 4 (moderate risk), the standard protocol is to admit for observation, serial EKGs, and cardiac biomarkers.
Diagnostics & Findings
- Review of EMS 12-lead EKG (interpreted as negative)
- HEART Score calculation (Score: 4)
Findings:
- Ongoing chest pain despite 4mg Morphine and sublingual nitro.
Interventions
- Administered 324 mg chewable aspirin
- Planned admission for new onset angina
⮑ Outcome & Reassessment
Pain minimally relieved by initial medications. Scheduled for admission to telemetry/med-surg.
Clinical Media

Cardiac Arrest & Resuscitation
Dr. Robby observes improper EKG lead placement; patient suddenly loses pulse.
+1
Cardiac Arrest & Resuscitation
Dr. Robby observes improper EKG lead placement; patient suddenly loses pulse.
Medical Decision Making
Robby notices the anterior EKG leads are placed too low, a common error made by medics trying to avoid female breast tissue. Immediately after this observation, the patient arrests into ventricular tachycardia. Standard ACLS protocol dictates immediate defibrillation for pulseless V-Tach.
Diagnostics & Findings
- Visual inspection of EKG lead placement
- Cardiac monitor rhythm check (V-Tach)
Findings:
- Anterior leads placed too inferiorly
- Loss of pulse, V-Tach on monitor
Interventions
- Defibrillator charged to 200 Joules
- Delivered single synchronized/unsynchronized shock
⮑ Outcome & Reassessment
Return of Spontaneous Circulation (ROSC) achieved immediately after one shock. Patient returned to normal sinus rhythm with a strong pulse. Ordered a repeat 12-lead EKG with proper lead placement.
Clinical Media

Post-Resuscitation Care & Cath Lab Transfer
Evaluation of repeat EKG post-cardiac arrest.
+2
Post-Resuscitation Care & Cath Lab Transfer
Evaluation of repeat EKG post-cardiac arrest.
Medical Decision Making
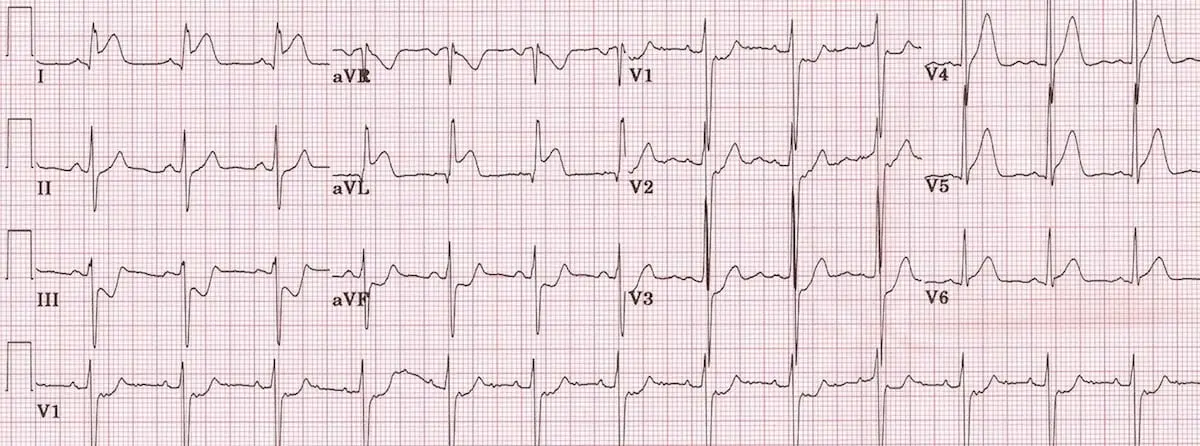
With leads correctly placed under the breast tissue, the EKG clearly shows a lateral STEMI. The ischemic myocardium triggered the V-Tach. The patient requires emergent percutaneous coronary intervention (PCI).
Diagnostics & Findings
- Repeat 12-lead EKG
Findings:
- Massive lateral STEMI evident on properly placed EKG.
Interventions
- Activated Code STEMI
- Left defibrillator pads on patient
- Arranged immediate transport to Cath Lab
⮑ Outcome & Reassessment
Patient is conscious, scared, and reports feeling 'like I got kicked in the chest' (expected after defibrillation). Pain is down to an 8.
Clinical Media
Case Review / Provider Education
Dr. Robby confronts the pre-hospital medics regarding their procedural error.
Case Review / Provider Education
Dr. Robby confronts the pre-hospital medics regarding their procedural error.
Medical Decision Making
Robby identifies that the medics prioritized the patient's modesty over diagnostic accuracy, leading to a false-negative EKG and a near-fatal cardiac arrest.
Diagnostics & Findings
Findings:
- Confirmed medics placed leads too inferiorly because they were afraid to move the patient's breasts.
Interventions
- Educated medics on the life-threatening danger of modifying EKG lead placement to avoid undergarments.
⮑ Outcome & Reassessment
Patient was already in the Cath lab.
Diagnoses & Disposition
Evolving Diagnoses
- [00:13:46]New Onset Angina / NSTEMI
- [00:15:28]Pulseless Ventricular Tachycardia (V-Tach)
- [00:18:29]Massive Lateral STEMI
Current Disposition
Transferred to Cardiac Cath Lab for emergent PCI.
Casebook Analysis
Episode Context
The case functions as a sharp, high-stakes medical vignette that highlights the dangerous real-world gender disparities in cardiac care. It also serves to showcase Dr. Robby's sharp clinical eye and uncompromising standards right before he contemplates leaving the hospital.
Attending's Review
Medical Accuracy
Highly accurate and clinically relevant. EKG lead malposition specifically placing V4, V5, and V6 too low to avoid female breast tissue is a pervasive issue in emergency medicine. This exact error frequently obscures anterior and lateral ischemic changes. The progression from an untreated occlusive myocardial infarction to unstable Ventricular Tachycardia, and the successful conversion with a 200J shock, is an excellent depiction of ACLS protocols.
Complications & Errors
- Pre-hospital medics placed anterior/lateral EKG leads too inferiorly to avoid moving the patient's breast tissue, generating a false-negative EKG.
Clinical Pearls
Always physically verify EKG lead placement, especially in female or obese patients. Leads V4-V6 must be placed in the 5th intercostal space, which routinely requires lifting breast tissue.
When evaluating for Acute Coronary Syndrome, a complete 12-lead EKG is strictly required over limited 8-lead or standard telemetry monitoring. Limited lead setups lack the full spatial resolution necessary to accurately detect localized ischemic changes, particularly in the lateral and posterior walls, and often fail to capture the reciprocal depressions essential for confirming acute occlusion.
A 'normal' EKG in the setting of ongoing, nitro-refractory chest pain is not entirely reassuring and requires serial EKGs.
A lateral STEMI is identified by ST elevation in leads I, aVL, V5, and V6, frequently with reciprocal ST depression in leads II, III, and aVF. Missing this requires immediate correction of lead placement.
Do not hesitate to remove clothing or undergarments to obtain a diagnostic-quality 12-lead EKG. Patient modesty should never supersede life-saving diagnostics.