History of Present Illness
18-year-old college student found unresponsive in his bed by his mother. No known medical history, no daily medications, no known allergies. Found barely breathing with pinpoint pupils and a heart rate of 38. Prehospital EMS administered Narcan which improved pupillary response, but the patient failed to breathe spontaneously and required endotracheal intubation. No obvious signs of trauma, and no drugs or alcohol were reported on the scene. Later collateral history from a classmate revealed he had volunteered to pick up illicit 'Xanax' for a study group to help them sleep, confirming a counterfeit pill ingestion resulting in a massive fentanyl overdose.

Emergency Department Course
Initial Evaluation & Resuscitation
Patient arrival via EMS, unresponsive and intubated.
+1
Initial Evaluation & Resuscitation
Patient arrival via EMS, unresponsive and intubated.
Medical Decision Making
Considering toxidromes vs. primary neurologic event vs. trauma. Opiate overdose fits the initial pinpoint pupils, but failure to regain respiratory drive post-Narcan suggests prolonged hypoxia leading to brain injury. Beta blockers wouldn't explain the pinpoint pupils. Need to evaluate brainstem reflexes to determine the extent of neurologic damage.
Diagnostics & Findings
- Pupillary exam
- Pain stimulus response check
Findings:
- Pupils 6mm and non-reactive
- No response to pain
- GCS 3
Interventions
- Mechanical ventilation (continued from EMS)
⮑ Outcome & Reassessment
Patient remains deeply comatose, flaccid, and unresponsive.
Clinical Media
Neurological Reassessment
Continuing primary survey to establish a neurologic baseline before CT scan.
+1
Neurological Reassessment
Continuing primary survey to establish a neurologic baseline before CT scan.
Medical Decision Making
With a GCS of 3 and fixed/dilated pupils, Dr, Robby needs to check for remaining brainstem function. The oculovestibular reflex (cold caloric test) tests the integrity of the brainstem. The absence of response confirms severe hypoxic injury or massive intracranial hemorrhage.
Diagnostics & Findings
- Ice water caloric test (oculovestibular reflex)
Findings:
- Flaccid paralysis of all four extremities
- No eye movement with ice water
Interventions
- Preparation for transport to CT scanner
⮑ Outcome & Reassessment
Patient demonstrates total absence of brainstem reflexes. Sent to CT with a drug box and continuous monitoring.
Clinical Media

Lab Review & Family Education
Return of Head CT results and Urine Drug Screen (UDS). Parents present at bedside.
Lab Review & Family Education
Return of Head CT results and Urine Drug Screen (UDS). Parents present at bedside.
Medical Decision Making
Head CT is normal, which rules out massive hemorrhage and confirms anoxic brain injury as the cause of brainstem failure. UDS is positive for fentanyl, explaining the initial respiratory arrest. Need to educate the family that fentanyl is frequently found in counterfeit prescription pills (like Xanax or Ativan), which explains why an otherwise 'good kid' suffered an opioid overdose.
Diagnostics & Findings
- Head CT
- Urine Drug Screen (UDS)
Findings:
- Head CT: Normal (no acute intracranial hemorrhage)
- UDS: Positive for Fentanyl
Interventions
- Family counseling and emotional support
⮑ Outcome & Reassessment
Patient condition unchanged. Parents initially in denial regarding drug use, but accept the information and are allowed to sit at the bedside.
End of Life / Brain Death Declaration Prep
Patient has had sufficient time for toxins to clear (with Narcan) but shows no neurologic recovery. Need to formalize the poor prognosis.
End of Life / Brain Death Declaration Prep
Patient has had sufficient time for toxins to clear (with Narcan) but shows no neurologic recovery. Need to formalize the poor prognosis.
Medical Decision Making
The clinical picture of absent cranial nerve activity and blown pupils following an anoxic event is practically diagnostic of brain death. However, strict legal and medical protocols require formal confirmatory testing to declare death: an apnea test and a cerebral perfusion study. Must prepare the family for the reality that their son will not wake up.
Diagnostics & Findings
- Ongoing serial neurologic exams
Findings:
- No cranial nerve activity
Interventions
- Discussed need for apnea test and cerebral perfusion study
- Delivered grave news to the parents
⮑ Outcome & Reassessment
Patient remains clinically brain-dead. The mother demonstrates severe grief and bargaining, pleading for the doctor to 'shock him back' and wake him up.
Apnea Test Initiation
Executing the formal brain death testing protocol discussed with the family.
+1
Apnea Test Initiation
Executing the formal brain death testing protocol discussed with the family.
Medical Decision Making
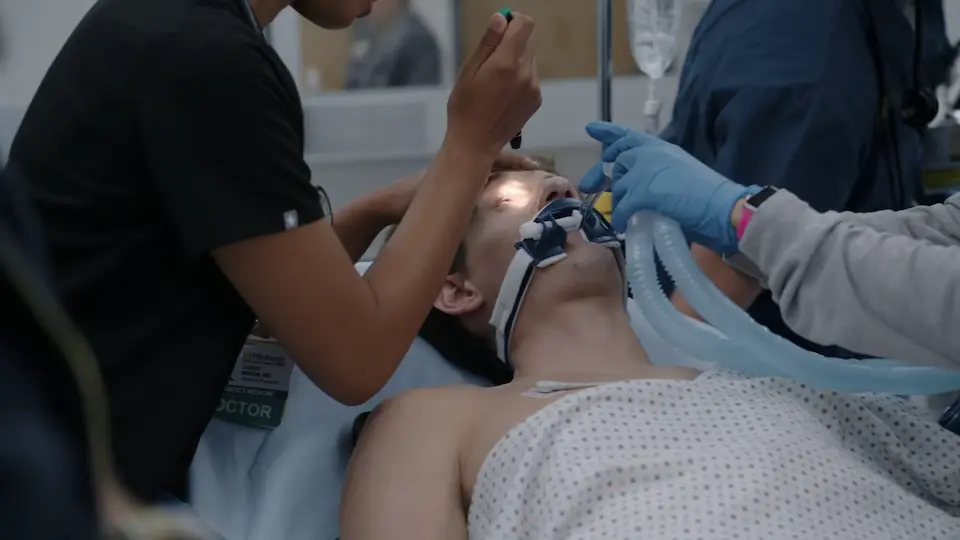
To formally diagnose brain death, we must prove the brainstem has lost its respiratory drive. The Apnea Test involves pre-oxygenating the patient with 100% O2, pausing the ventilator's breaths for 10 minutes, and monitoring for any spontaneous respiratory effort. We then draw an ABG to measure PaCO2; if it rises significantly (typically >60 mmHg or 20 mmHg above baseline) without triggering a breath, the brainstem is definitively non-functional.
Diagnostics & Findings
- Apnea Test
Findings:
- No spontaneous respirations observed during 10-minute vent pause
Interventions
- Administered 100% Oxygen
- Paused mechanical ventilator breaths
⮑ Outcome & Reassessment
Patient exhibited zero respiratory effort. Blood drawn for Arterial Blood Gas (ABG) to quantify CO2 accumulation.
Clinical Media

Apnea Test Results & Next Steps
ABG results return from the lab following the Apnea Test.
+1
Apnea Test Results & Next Steps
ABG results return from the lab following the Apnea Test.
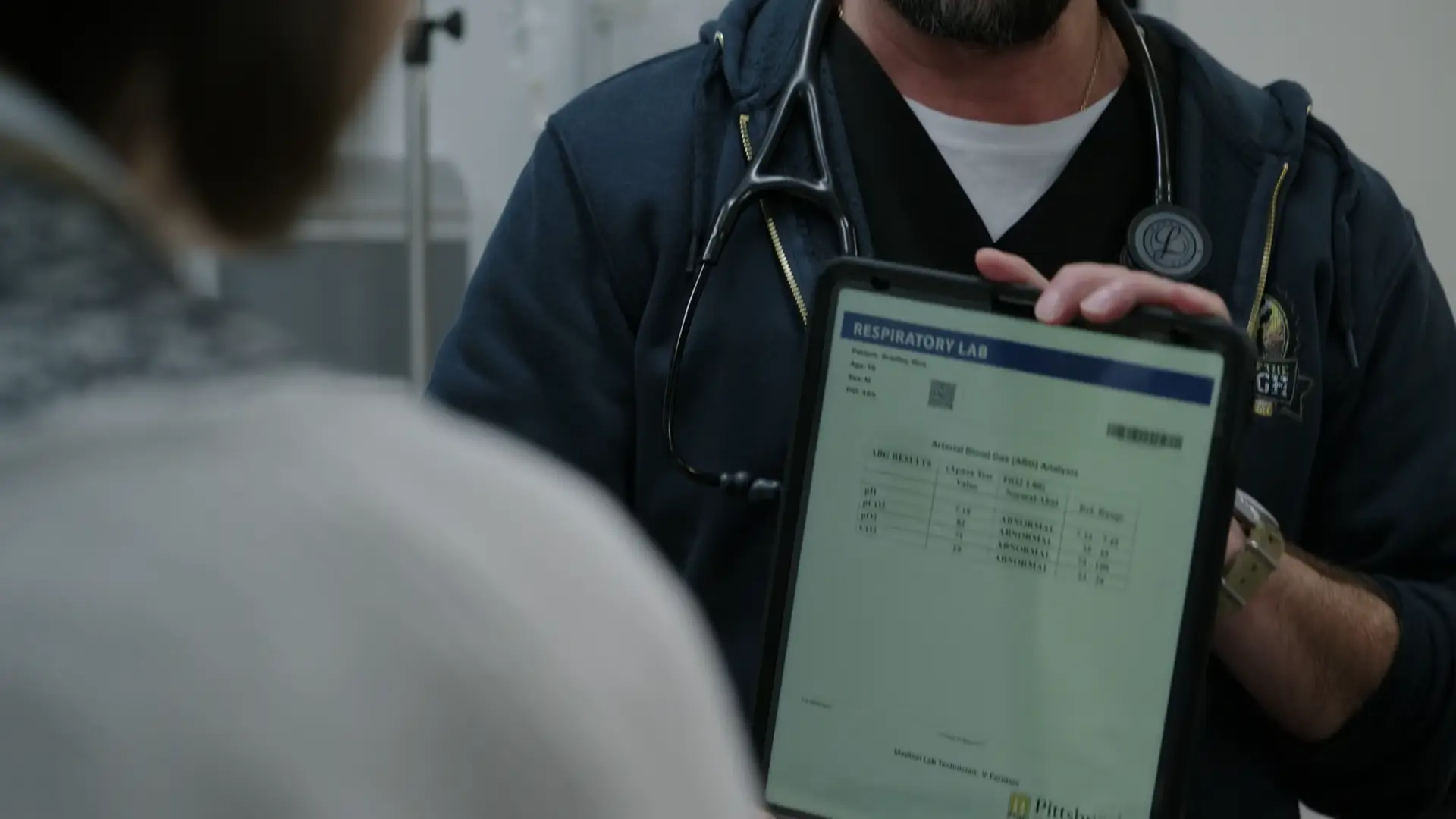
Medical Decision Making
The ABG shows a PaCO2 of 82. Normal is 35-45, and a level above 60 without a respiratory response is a positive test for brain death. The parents are still struggling to accept this. To provide absolute, undeniable proof and fulfill final institutional criteria, Dr. Robinavitch will order a Cerebral Perfusion Study.
Diagnostics & Findings
- Arterial Blood Gas (ABG) interpretation
Findings:
- PaCO2: 82 mmHg (Positive Apnea Test)
Interventions
- Ordered Cerebral Perfusion Study (Nuclear Medicine)
- Extensive family counseling on test implications
⮑ Outcome & Reassessment
Diagnosis of brainstem death clinically confirmed. The family requests the final confirmatory imaging study.
Clinical Media
Social Work & OPO Coordination
Preparing the family for the finality of the cerebral perfusion study and initiating end-of-life/organ donation pathways.
Social Work & OPO Coordination
Preparing the family for the finality of the cerebral perfusion study and initiating end-of-life/organ donation pathways.
Medical Decision Making
Medical management has concluded, but psychological management of the family is peaking. Dr. Robinavitch calls for Kiara to provide dedicated bereavement counseling. Furthermore, as brain death is confirmed, the patient is an ideal candidate for organ donation. An Organ Procurement Organization (OPO) transplant counselor will need to evaluate, but the family must be primed and emotionally supported first.
Diagnostics & Findings
Interventions
- Consulted Social Work (Kiara)
- Initiated preliminary Organ Donation evaluation pathway
⮑ Outcome & Reassessment
Patient remains boarded in Central 7 pending Nuclear Medicine scan and OPO family approach.
Ancillary Brain Death Testing
Nuclear Medicine is ready to perform the cerebral perfusion study.
Ancillary Brain Death Testing
Nuclear Medicine is ready to perform the cerebral perfusion study.
Medical Decision Making
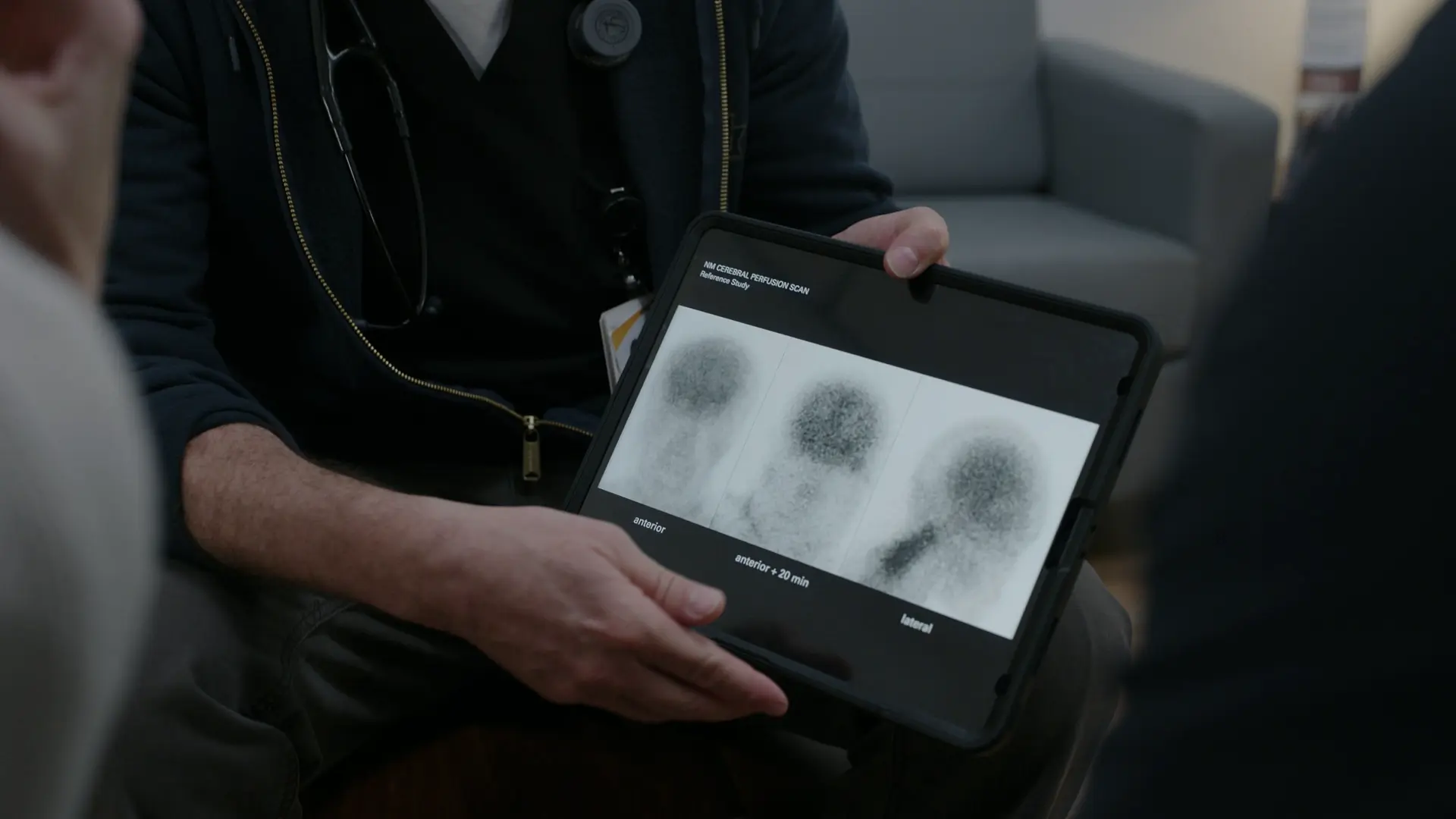
To formally finalize brain death documentation and provide undeniable proof for the grieving family (who remain in profound denial), the ancillary cerebral perfusion study is initiated. The test involves injecting a radiopharmaceutical to evaluate cerebral blood flow; absence of uptake in the brain confirms brain death. The family needs guidance on the logistics and safety protocols (radiation precautions) of the test.
Diagnostics & Findings
- Cerebral Perfusion Study (Transported)
Findings:
- Awaiting results (estimated 1 hour)
Interventions
- Coordinated transport to Nuclear Medicine
- Counseled parents on test logistics and radiation safety
⮑ Outcome & Reassessment
Patient transported to Nuclear Medicine. The parents exhibit continued severe denial, expressing belief that Nick will 'pull through'.
Brain Death Confirmation
Cerebral perfusion study results return from Nuclear Medicine.
+2
Brain Death Confirmation
Cerebral perfusion study results return from Nuclear Medicine.
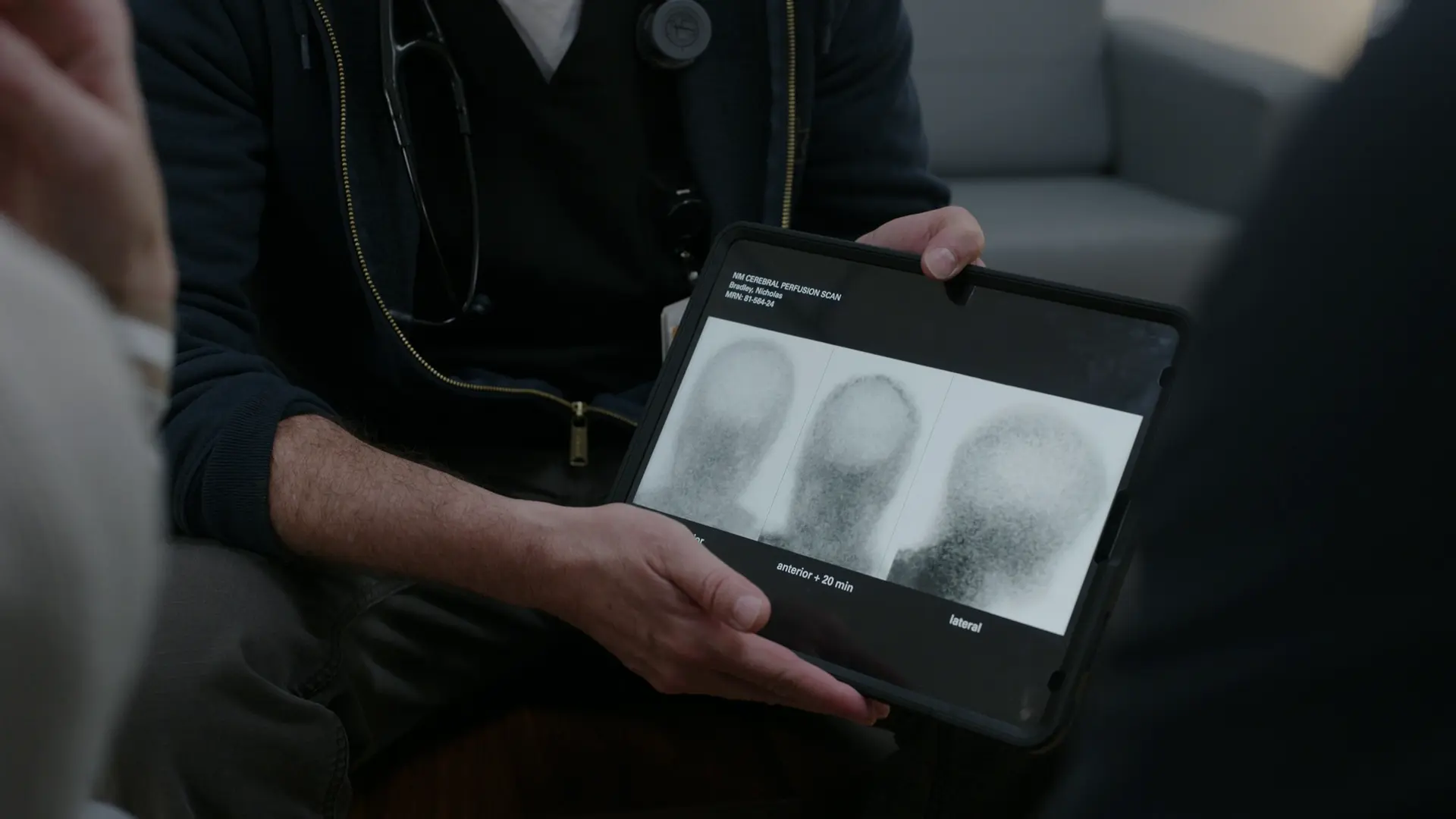
Medical Decision Making
The cerebral perfusion scan confirms absolutely no blood flow to the cerebrum or brain stem. This definitively satisfies the criteria for brain death. Dr, Robby must communicate this to the parents using visual evidence to help break through their denial, then transition their care to the OPO team.
Diagnostics & Findings
- Cerebral Perfusion Study interpretation
Findings:
- No cerebral or brain stem blood flow
Interventions
- Delivered definitive brain death diagnosis to parents
- Utilized visual scan comparison for family comprehension
- Contacted CORE (Center for Organ Recovery & Education) / Family Support Specialist
⮑ Outcome & Reassessment
Patient is formally declared dead. Parents are devastated but the undeniable visual proof begins to dismantle their denial.
Clinical Media
Organ Donation Counseling
Transitioning care to the Organ Procurement Organization (OPO) to discuss donation.
Organ Donation Counseling
Transitioning care to the Organ Procurement Organization (OPO) to discuss donation.
Medical Decision Making
The medical team's role in treating the patient has ended. Best practice dictates that a trained OPO counselor approaches the family regarding organ donation to prevent any perceived conflict of interest. Nick is a registered donor on his driver's license (first-person consent), but his grieving parents may struggle to honor this wish. The OPO counselor must navigate this delicate ethical and emotional terrain.
Diagnostics & Findings
Findings:
- Patient identified as a registered organ donor on state ID/driver's license
Interventions
- Introduced OPO counselor/Family Support Specialist
- Initiated discussion on funeral arrangements and organ donation wishes
⮑ Outcome & Reassessment
Parents express strong resistance to organ donation despite Nick's registered status, arguing he was 'too young' to make that decision. Given time to process by the OPO counselor.
Diagnoses & Disposition
Evolving Diagnoses
- [S01E02]Opiate Overdose (Fentanyl)
- [S01E02]Severe Hypoxic-Ischemic Encephalopathy (Anoxic Brain Injury)
- [S01E02]Clinical Brain Death
- [S01E03]Positive Apnea Test (PaCO2 82)
- [S01E04]Clinical Brain Death (Pending Ancillary Confirmation)
- [S01E06]Confirmed Brain Death (Absent Cerebral Perfusion)
Current Disposition
Formally declared brain dead following a cerebral perfusion study showing absent cerebral blood flow. Currently maintained on somatic support while the family discusses his registered organ donor status with the Organ Procurement Organization (OPO) counselor.
Casebook Analysis
Episode Context
Nick's case spans multiple episodes, operating as a tragic emotional anchor that highlights the pervasive nature of the modern fentanyl epidemic. In S1E3, the storyline shifts from acute resuscitation to the agonizing process of grieving, brain death declaration, and the ethical/logistical challenges of boarding deceased patients in the ED. In S1E4, the collateral emotional damage is explored as Jenna, a classmate involved in sourcing the counterfeit Xanax, apologizes to Nick's father. In S1E6, the cerebral perfusion scan returns showing absent blood flow, confirming brain death and extinguishing the parents' lingering denial. The narrative transitions entirely to the delicate, ethically fraught process of organ procurement, exploring the conflict between Nick's legal first-person authorization (his driver's license registry) and his parents' fierce, grief-stricken resistance to the donation.
Attending's Review
Medical Accuracy
The depiction of brain death testing is exceptionally accurate. The parameters of the Apnea Test keeping the patient on 100% oxygen to prevent hypoxia while stopping the ventilator to allow CO2 to rise are correct. The threshold quoted (a PaCO2 rising above 60 mmHg) is the factual real-world benchmark for confirming an absent respiratory drive. Following up with a Cerebral Perfusion Study as a confirmatory ancillary test is standard practice when families struggle to accept the clinical diagnosis. Using a cerebral perfusion scan (Nuclear Medicine) showing the 'hollow skull' or 'empty lightbulb' sign (white/no uptake) is highly accurate for visually demonstrating absent cerebral blood flow to families. Also, the involvement of a specialized OPO counselor (Emma) to decouple the death declaration from the donation request is an accurate reflection of best practices.
Complications & Errors
- There were no medical errors made by the ED team. The tragic outcome was entirely secondary to the prolonged anoxic downtime before the patient was discovered by his parents.
Clinical Pearls
Naloxone (Narcan) reverses the opioid toxidrome at the receptor level, but it cannot reverse anoxic brain injury sustained during prolonged respiratory depression.
The oculovestibular reflex (ice water caloric test) is a crucial, easily performed bedside test to evaluate lower brainstem function in comatose patients.
During an Apnea Test, the patient is pre-oxygenated and disconnected from the ventilator. An Arterial Blood Gas (ABG) showing a PaCO2 > 60 mmHg (or 20 mmHg above baseline) without any respiratory effort confirms absent medullary drive.
The Apnea Test is a legally significant procedure that requires strict prerequisites, including normothermia (core temp ≥ 36°C) and hemodynamic stability (SBP ≥ 100 mmHg). The test must be immediately aborted if the patient experiences significant desaturation (SpO2 < 85%) or cardiovascular collapse, drawing a stat ABG at the time of abort to check if the PaCO2 target was already reached.
Ancillary testing for brain death, such as a Nuclear Medicine Cerebral Perfusion Study, is indicated when clinical testing cannot be fully completed, or to provide definitive visual proof for families struggling with acceptance.
The Emergency Department often plays a critical role in organ donation; stabilizing a brain-dead patient in the ED rather than rushing them out allows OPO counselors the time to properly approach grieving families.
Visualizing the 'hollow skull' or 'empty lightbulb' sign on a radionuclide cerebral perfusion scan provides undeniable, objective evidence of brain death, which can be highly effective in helping grieving families accept the prognosis.
Best practice in end-of-life care mandates uncoupling the delivery of the death notification (done by the physician) from the request for organ donation (done by a specialized OPO counselor). This prevents families from feeling the medical team 'gave up' to harvest organs.
First-person authorization (e.g., a donor registry on a driver's license) is legally binding in most US states, but OPO teams still prioritize working collaboratively with families to gain their emotional support rather than strictly enforcing the legal mandate against their wishes.


