History of Present Illness
Adult male brought in by flight crew after sustaining a high-voltage electrical injury to his left forearm. He was found at an abandoned factory with bolt cutters at his side, suggesting he cut into a live wire while attempting to steal copper. Pre-hospital course was complicated by a witnessed ventricular fibrillation (V-fib) arrest requiring at least one defibrillation shock prior to ED arrival.

Emergency Department Course
Initial Resuscitation & Cardiac Arrest
Patient arrival via helicopter EMS following high-voltage electrocution.
+1
Initial Resuscitation & Cardiac Arrest
Patient arrival via helicopter EMS following high-voltage electrocution.
Medical Decision Making
High-voltage electrocution causes massive internal muscle necrosis leading to rhabdomyolysis and subsequent acute kidney injury (AKI). The immediate threats are cardiac arrhythmias (recurrent V-fib) from the electrical shock and hyperkalemia secondary to muscle breakdown. The tense ventral compartment of the forearm raises immediate concern for acute compartment syndrome.
Diagnostics & Findings
- Continuous cardiac monitoring
- CK (Creatine Kinase)
- Myoglobin
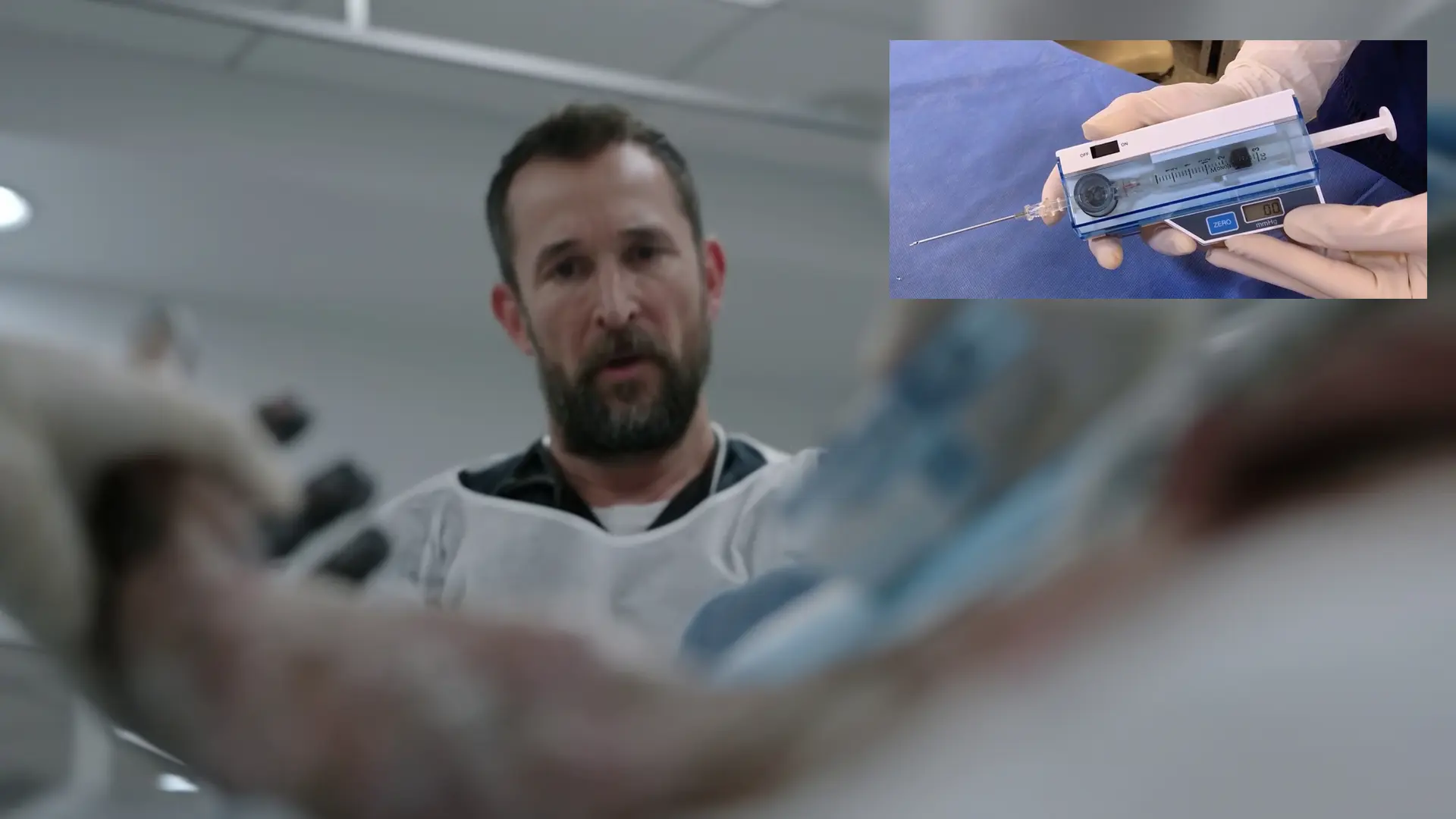
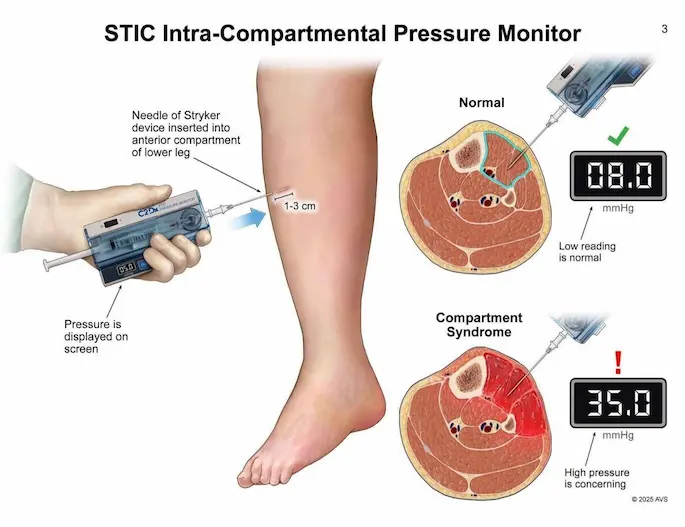
- STIC pressure monitor setup
Findings:
- Tense ventral compartment on left forearm
- Patient acutely decompensates into Ventricular Fibrillation
Interventions
- 2 Liters Normal Saline wide open
- AP (Anteroposterior) Defibrillator pads placed
- Defibrillation at 300 Joules
⮑ Outcome & Reassessment
Patient was shocked at 300J for V-fib. Rhythm converts, but forearm swelling worsens.
Clinical Media

Bedside Procedure
Reassessment of the left forearm burn and swelling.
+3
Bedside Procedure
Reassessment of the left forearm burn and swelling.
Medical Decision Making
STIC monitor indicates an interior compartment pressure of 49 mmHg. Normal pressure is < 10 mmHg; > 30 mmHg is an absolute indication for surgical decompression. Although the radial pulse is still palpable (which requires pressures near 100 mmHg to occlude), 49 mmHg is high enough to cause irreversible ischemic necrosis of the nerves and muscles within hours. An emergent bedside fasciotomy is required to salvage the limb before definitive OR washout.
Diagnostics & Findings
- STIC Compartment Pressure Measurement (Result: 49 mmHg)
- Radial pulse check
Findings:
- Massive swelling due to deep tissue burn
- Compartment pressure critically elevated at 49 mmHg
- Intact radial pulse
Interventions
- Bedside Volar/Ventral Forearm Fasciotomy
- Incision made proximally avoiding the median nerve and major vessels
- Orthopedics consulted for definitive OR completion
⮑ Outcome & Reassessment
Incision successfully relieves immediate tension; patient prepped for Orthopedics in the OR.
Clinical Media

Diagnoses & Disposition
Evolving Diagnoses
- [00:30:00]High-Voltage Electrical Injury
- [00:30:00]Ventricular Fibrillation
- [00:30:00]Rhabdomyolysis
- [00:35:35]Acute Compartment Syndrome (Left Forearm)
Current Disposition
Transferred to the Operating Room for Orthopedic/Trauma management of the fasciotomy and electrical burn.
Casebook Analysis
Episode Context
The case serves as a high-adrenaline trauma beat that highlights the clinical competence of the ED staff while providing a teaching moment furthering Dr. Santos's and Dr. Garcia's developing relationship. Attending physicians use the critical presentation to drill Santos on the pathophysiology of rhabdomyolysis and guide her through a bedside fasciotomy.
Attending's Review
Medical Accuracy
The medical depiction is highly accurate. High-voltage injuries frequently cause deep muscle necrosis sparing superficial tissue, leading directly to massive rhabdomyolysis and compartment syndrome. Fluid resuscitation (2L NS wide open) and checking CK/myoglobin are standard of care. The discussion around compartment syndrome is exceptionally realistic: the team correctly notes that a pressure of 49 mmHg necessitates decompression, and they explicitly mention that you do not wait for the loss of a pulse to diagnose compartment syndrome. Bedside fasciotomies in the ED are rare but indicated if the OR is delayed.
Clinical Pearls
Compartment Syndrome Dx: The forearm is divided by fascia into two main compartments: ventral (anterior) and dorsal (posterior). High-voltage electrocution often causes severe tetanic contractions that force victims to grip the electrical source, preventing them from letting go. This prolonged current exposure leads to deep muscle necrosis and massive swelling specifically in the ventral compartment.
A compartment pressure >30 mmHg (or a Delta P <30) mandates emergent fasciotomy. Waiting for the loss of pulses is a dangerous pitfall, as pulses remain intact long after microvascular perfusion has ceased.
The 'Iceberg Effect' in electrical burns: Skin findings severely underestimate the extent of deep tissue destruction. Aggressive IV fluid resuscitation is necessary to flush myoglobin and prevent acute kidney failure.
Loss of a pulse is a very late and often irreversible sign of Compartment Syndrome. Diagnosis relies on clinical suspicion (pain out of proportion, tense compartments) and compartment pressure measurements > 30 mmHg.
Volar Forearm Fasciotomy Incision Design: A straight-line incision is a critical error when decompressing the forearm. The incision must utilize a curvilinear or 'lazy-S' approach to safely avoid the median nerve and radial/ulnar arteries, and must cross joint flexion creases diagonally to prevent permanent, mobility-limiting scar contractures.
Similar Cases from The Show



Chart Navigation
Unknown
C/OHigh-voltage electrocution and ventricular fibrillation