History of Present Illness
23-year-old male arrives via EMS after getting 'doored' while riding an e-scooter without a helmet. Mechanism of injury involves his neck striking the handlebar, followed by a face-plant onto the pavement. He complains of blood pooling in the back of his throat.

Emergency Department Course
Trauma Arrival & Initial Resuscitation
Patient arrival as a Tier 1 code trauma.
+3
Trauma Arrival & Initial Resuscitation
Patient arrival as a Tier 1 code trauma.
Medical Decision Making
Patient is tachycardic and borderline hypoxic with significant epistaxis leading to posterior pharyngeal blood pooling. Physical exam reveals a 'floating face' indicative of a Le Fort III fracture and a shifted larynx. The high risk of airway loss dictates a 'double setup' (preparing for both oral intubation and a surgical airway simultaneously).
Diagnostics & Findings
- Primary trauma survey
- Airway assessment
- Laryngeal palpation
Findings:
- Alert and oriented
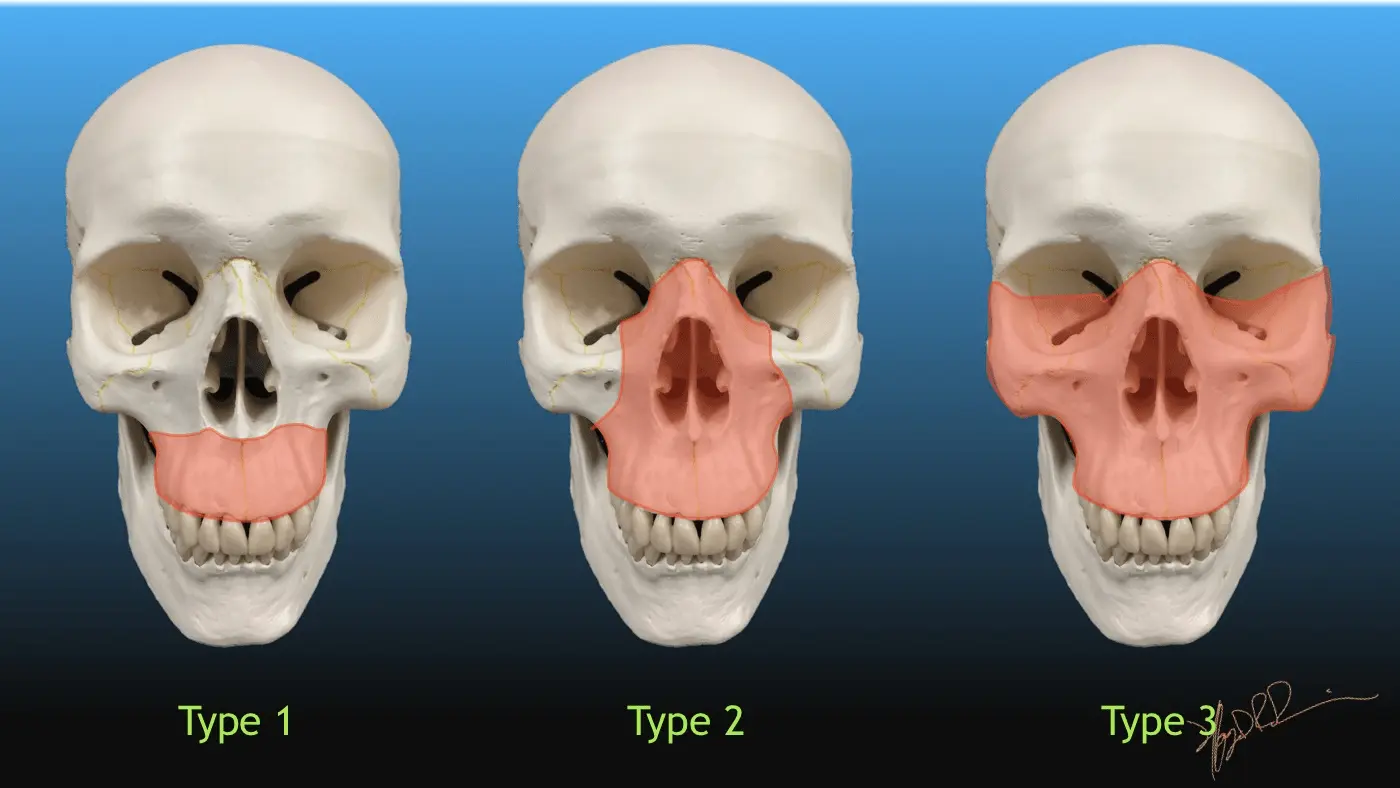
- Obvious facial fractures (Le Fort III)
- Larynx shifted to the right
- No crepitus
- No hemotympanum
Interventions
- Blow-by oxygen at 15L
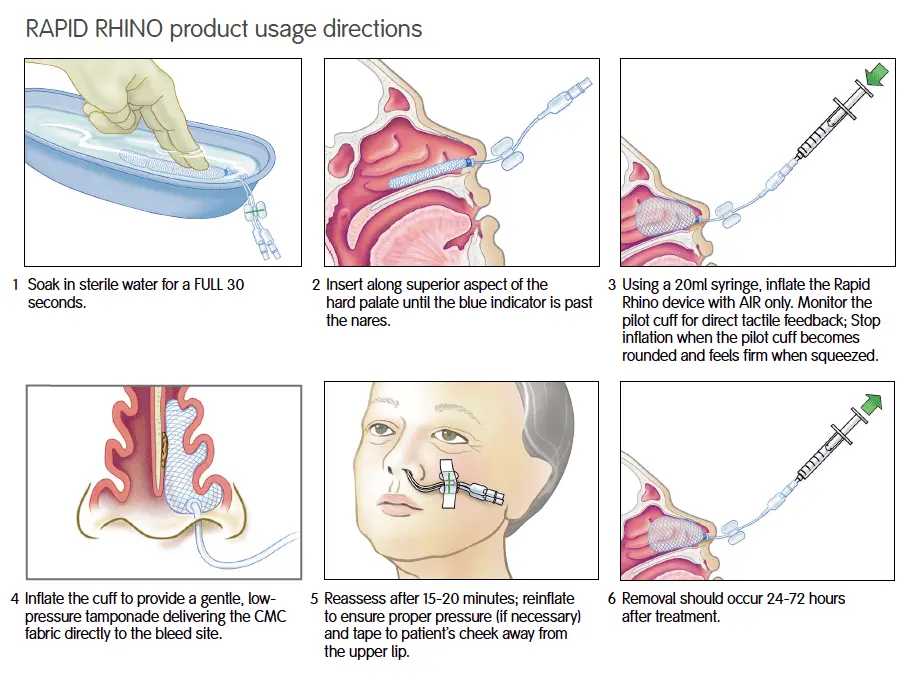
- Short Rapid Rhino insertion with balloon inflation to tamponade epistaxis
- Morphine 4mg IV for pain control
- Double setup prepared for airway management
⮑ Outcome & Reassessment
Epistaxis initially managed by the Rapid Rhino. Patient remains alert but requires definitive airway control due to escalating edema.
Clinical Media

Airway Crisis & Cricothyrotomy
Failure to visualize vocal cords during Rapid Sequence Intubation (RSI).
+2
Airway Crisis & Cricothyrotomy
Failure to visualize vocal cords during Rapid Sequence Intubation (RSI).
Medical Decision Making
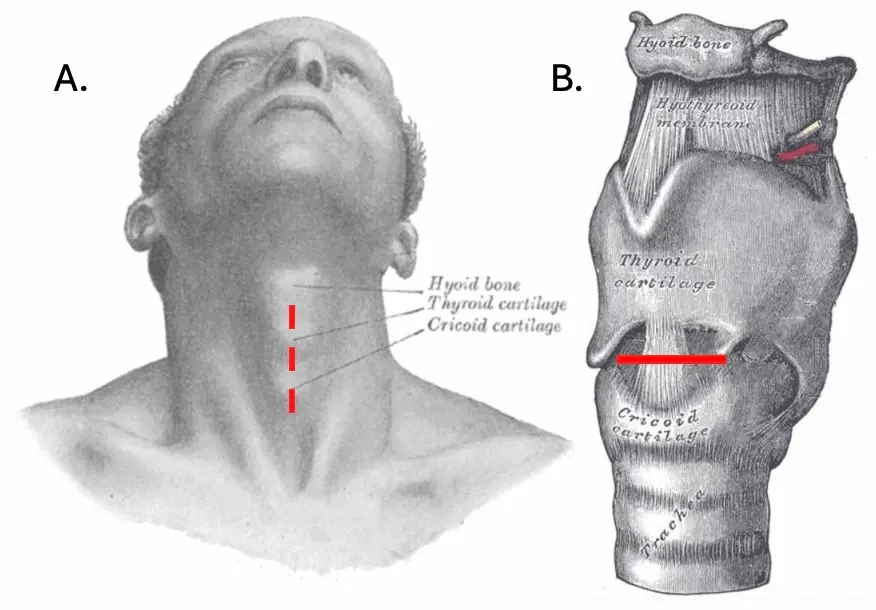
Direct laryngoscopy fails due to massive supraglottic swelling and anatomical distortion. With oxygen saturations dropping to 85%, this is a 'Cannot Intubate, Cannot Oxygenate' (CICO) scenario. A laryngeal fracture is a relative contraindication to a cricothyrotomy (as it can complete a partial transection), but the surgical resident correctly notes the contusion is high at the thyroid cartilage, making the cricothyroid membrane a safe surgical target. An I-gel is appropriately placed as a temporizing rescue airway to restore oxygenation before performing the open cricothyrotomy.
Diagnostics & Findings
- Direct laryngoscopy
- Continuous pulse oximetry monitoring
- End-tidal CO2 capnography
Findings:
- Massive edema obscuring vocal cords
- Desaturation to 85%
- Successful ventilation via I-gel
- Positive colorimetric capnography (yellow) confirming tracheal placement of the Shiley tube
Interventions
- RSI (Ketamine and Succinylcholine)
- Aborted direct laryngoscopy
- I-gel placement as a rescue airway
- Open cricothyrotomy (vertical skin incision, horizontal membrane incision)
- Insertion of 4.0 Shiley tracheostomy tube
- Initiation of Propofol drip for sedation
- Suturing the airway in place
⮑ Outcome & Reassessment
Oxygen saturations improved with the I-gel. The cricothyrotomy was successful with confirmed end-tidal CO2. The patient was stabilized and sent to CT.
Clinical Media

Diagnoses & Disposition
Evolving Diagnoses
- [Trauma Bay]Le Fort III Maxillofacial Fracture
- [Trauma Bay]Impending Airway Obstruction / CICO (Cannot Intubate, Cannot Oxygenate)
- [Trauma Bay]High Thyroid Cartilage Contusion
Current Disposition
Stabilized with a definitive surgical airway, sedated on a Propofol drip, and transferred for C-spine, Head CT, and Oral & Maxillofacial (OMF) Surgery consultation.
Casebook Analysis
Episode Context
This case functions as a high-adrenaline trauma set piece designed to showcase the intense rivalry and territorial disputes between the Emergency Medicine and General Surgery departments. It also serves as a critical rite of passage for Mel, who steps up to successfully perform her first live surgical airway under extreme pressure.
Attending's Review
Medical Accuracy
The execution of the airway crisis is clinically excellent. The team correctly recognizes the need for a 'double setup' in severe facial trauma. The debate over whether to perform a cricothyrotomy in the presence of a laryngeal contusion is highly accurate—cutting a fractured larynx can cause complete airway transection, but noting the injury was strictly high at the thyroid cartilage validates the decision. Using an I-gel as a bridging device to restore oxygenation before cutting is a textbook, modern CICO management strategy.
Complications & Errors
- The ER doctor almost attempts to intubate without optimizing the patient's pre-oxygenation status perfectly, though the rapid progression to a surgical airway mitigates this.
Clinical Pearls
In Le Fort II or III fractures, normal airway landmarks are often destroyed, and massive bleeding is guaranteed. Always prepare a surgical 'double setup' before pushing induction meds.
A vertical skin incision is preferred for a cricothyrotomy because it avoids the laterally located carotid arteries and jugular veins, even if you stray off the midline.
If you fail intubation, immediately drop in a supraglottic airway (like an LMA or I-gel) to temporize oxygenation. You do not have to perform a bloody surgical airway in a state of hypoxic panic if you can bag the patient through a rescue device first.


