History of Present Illness
Judith Lastrade is a G1P0 female at approximately 36-37 weeks gestation who presents via EMS with a 2-day history of a worsening headache, now rated 10/10, accompanied by blurred vision and significant pitting edema. She has had a 'wild pregnancy' with absolutely no prenatal care, intending to have a 'free birth' without medical intervention. Symptoms were completely refractory to pre-hospital fentanyl administration.

Emergency Department Course
Triage & EMS Handoff
Incoming critical patient alert
+1
Triage & EMS Handoff
Incoming critical patient alert
Medical Decision Making
Classic presentation for severe preeclampsia (severe hypertension, headache, visual changes, pitting edema in the third trimester). High risk for eclamptic seizure or stroke.
Diagnostics & Findings
- Pre-hospital vitals assessment
Findings:
- 10/10 headache, blurred vision, marked pitting edema, marked hypertension
Interventions
- Pre-hospital Fentanyl (failed to relieve headache)
⮑ Outcome & Reassessment
Symptoms refractory to fentanyl. Alerted ED for immediate severe preeclampsia management.
Clinical Media
Initial Assessment & Stabilization
Patient arrival in ED
+2
Initial Assessment & Stabilization
Patient arrival in ED
Medical Decision Making
Immediate priorities are blood pressure control to prevent stroke and administration of magnesium sulfate for seizure prophylaxis. Fetal monitoring is crucial to ensure fetal tolerance of the maternal condition.
Diagnostics & Findings
- Cardiotocography (CTG)
Findings:
- Fetal HR 128 (reassuring, normal range 110-160)
Interventions
- 6 grams Magnesium Sulfate IV bolus
- 20 mg Labetalol IV push over 2 minutes
⮑ Outcome & Reassessment
Patient resistant to medical explanation, desires only headache relief. Reassessment required as BP remains dangerously high.
Clinical Media


Reassessment & Bedside Ultrasound
Persistent 10/10 headache
+1
Reassessment & Bedside Ultrasound
Persistent 10/10 headache
Medical Decision Making
With no prenatal care, exact gestational age is unknown. Bedside ultrasound is needed to date the pregnancy to confirm viability for immediate delivery, which is the definitive treatment for severe preeclampsia.
Diagnostics & Findings
- Bedside Obstetric Ultrasound
Findings:
- Femur length 7 centimeters, correlating to approximately 37 weeks gestation
Interventions
- Fentanyl 50 mcg IV
- Additional 40 mg Labetalol IV push
⮑ Outcome & Reassessment
Patient refuses induction of labor despite explanation of risks (seizures, bleeding, fetal/maternal death).
Clinical Media

Clinical Deterioration & Seizure
Lab results return; Patient develops tonic-clonic seizure
+2
Clinical Deterioration & Seizure
Lab results return; Patient develops tonic-clonic seizure
Medical Decision Making
Diagnosis upgraded from Preeclampsia to Eclampsia. HELLP syndrome confirmed via labs. Seizure is causing maternal hypoxia and fetal bradycardia. Immediate seizure termination is required using benzodiazepines and secondary antiepileptics.
Diagnostics & Findings
- STAT Labs (CBC, CMP)
Findings:
- Hemoglobin 7.5 g/dL
- Platelets 40,000 /mcL
- Elevated LFTs (HELLP Syndrome)
Interventions
- 10 mg IV Diazepam (x2)
- 4 grams Keppra (Levetiracetam) IV push
- Magnesium infusion continued at 2g/hr
- 15L O2 via Non-Rebreather mask
⮑ Outcome & Reassessment
Seizure activity continues. Fetal heart rate drops to dangerous levels (~90 bpm). Maternal SpO2 drops to 88%. Intubation indicated.
Clinical Media

Airway Management & Refractory Seizure
Hypoxia and ongoing status epilepticus
+3
Airway Management & Refractory Seizure
Hypoxia and ongoing status epilepticus
Medical Decision Making
Rapid Sequence Intubation (RSI) needed for airway protection. Propofol chosen for its GABA-ergic anti-seizure properties. Succinylcholine chosen over Rocuronium to allow for rapid return of motor function, ensuring the team can identify ongoing non-convulsive seizures via EEG. Left Uterine Displacement (LUD) utilized to prevent aortocaval compression and optimize maternal/fetal hemodynamics.
Diagnostics & Findings
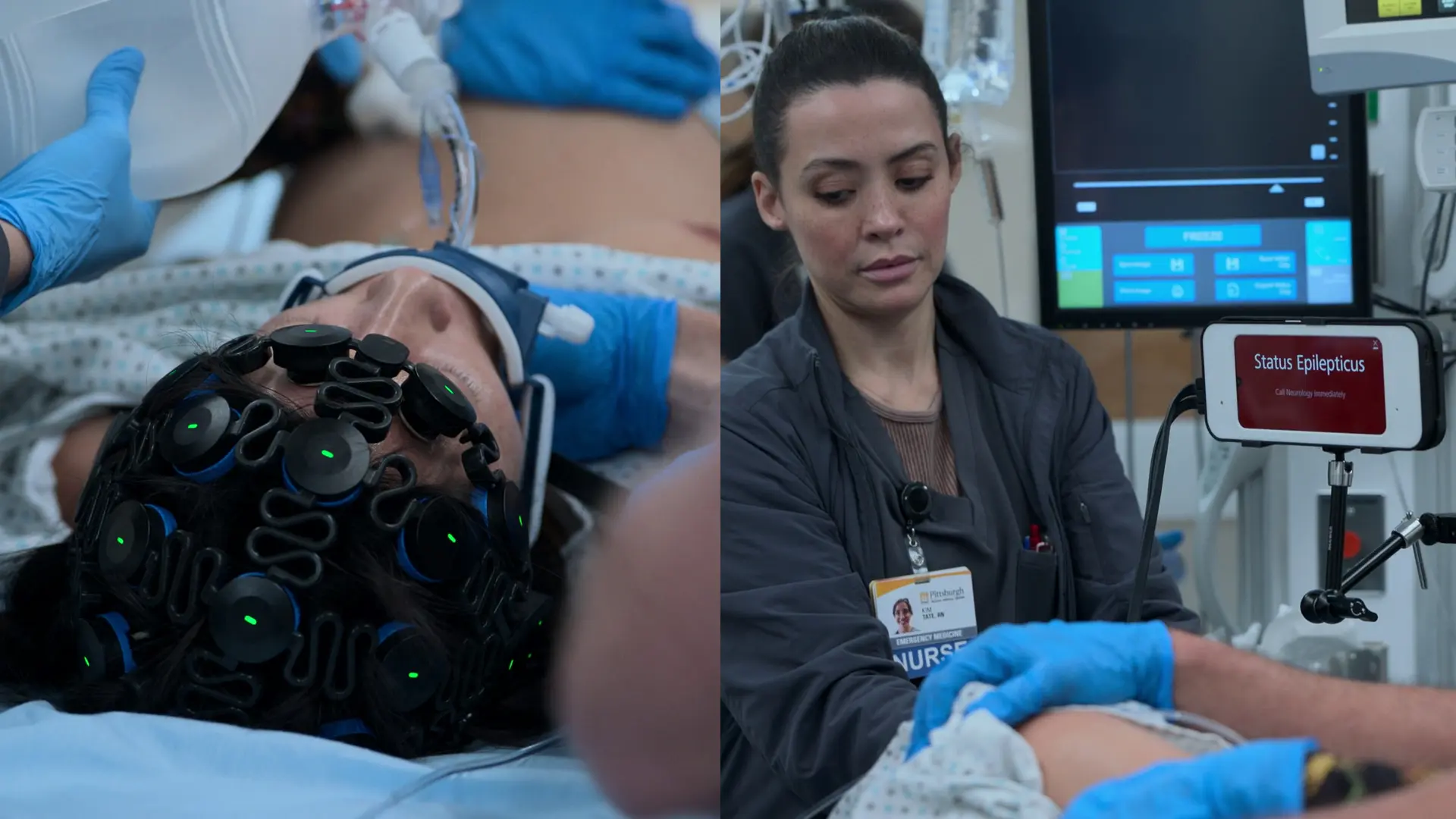
- Continuous EEG Monitoring
Findings:
- EEG confirms ongoing non-convulsive status epilepticus despite paralysis
Interventions
- 120 mg Propofol IV
- 60 mg Succinylcholine IV
- Endotracheal Intubation
- Left Uterine Displacement (Manual)
- 100 mg Ketamine IV push for refractory status
- O-Negative Blood Transfusion (Rapid Infuser)
- 10 mg Decadron (Dexamethasone) IV push
⮑ Outcome & Reassessment
Intubation successful. Seizure continues on EEG. Transfusion initiated due to HELLP anemia. Fetal heart rate temporarily improves to 104 bpm.
Clinical Media

Maternal Cardiac Arrest & Resuscitative Hysterotomy
Monitor alarms for Ventricular Fibrillation
+4
Maternal Cardiac Arrest & Resuscitative Hysterotomy
Monitor alarms for Ventricular Fibrillation
Medical Decision Making
Maternal cardiac arrest during third trimester triggers the '4-minute rule' for perimortem C-section (Resuscitative Hysterotomy). Delivery of the fetus is the ultimate resuscitative maneuver for the mother as it relieves aortocaval compression and increases venous return to the heart by up to 30%. Must incise rapidly despite severe thrombocytopenia.
Diagnostics & Findings
- Rhythm check (V-Fib)
Findings:
- Ventricular Fibrillation
- Breech presentation of fetus
Interventions
- High-quality CPR
- Defibrillation at 200J (x2)
- 1 mg Epinephrine IV
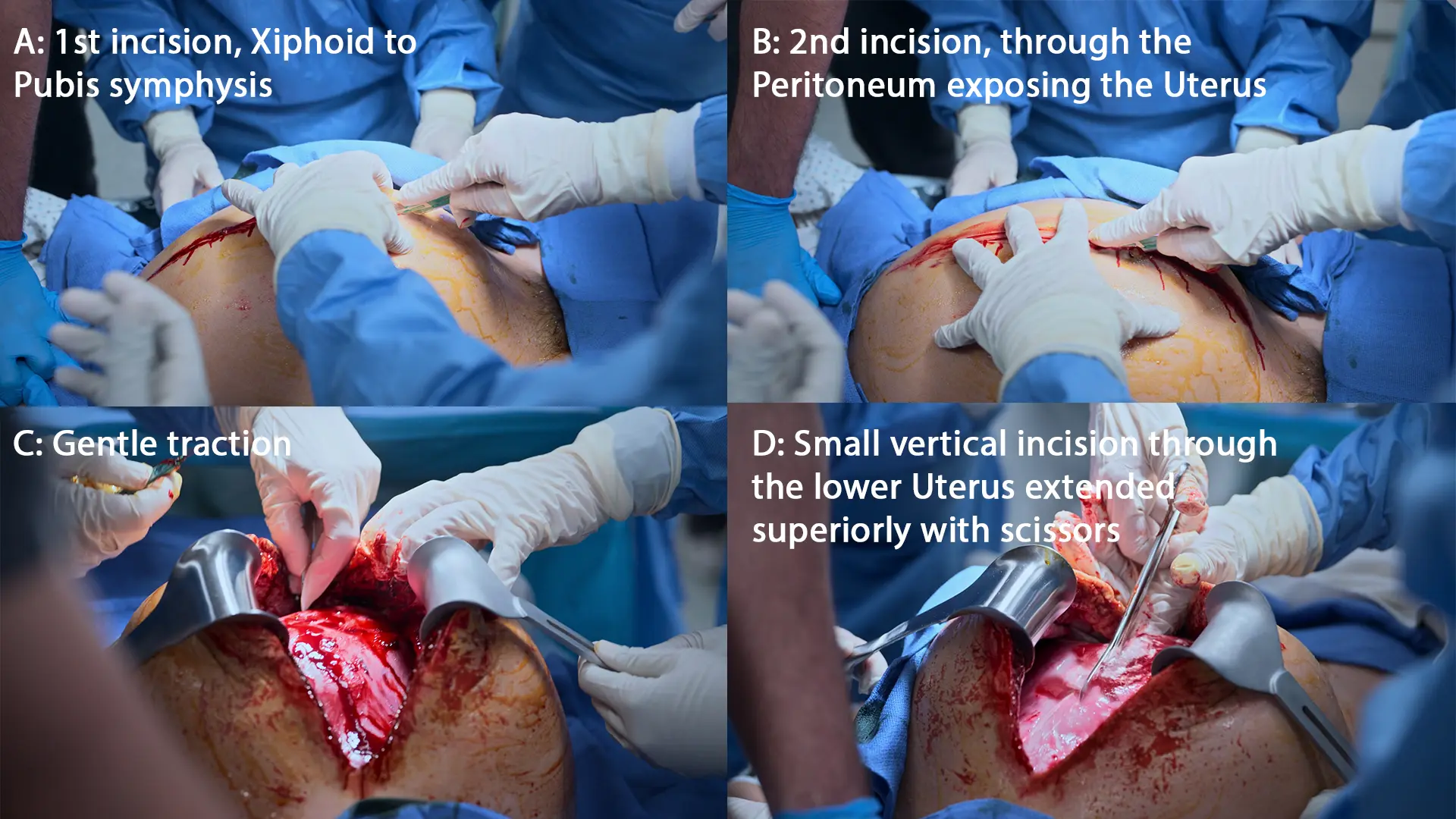
- Resuscitative Hysterotomy (Vertical xiphoid-to-pubis incision)
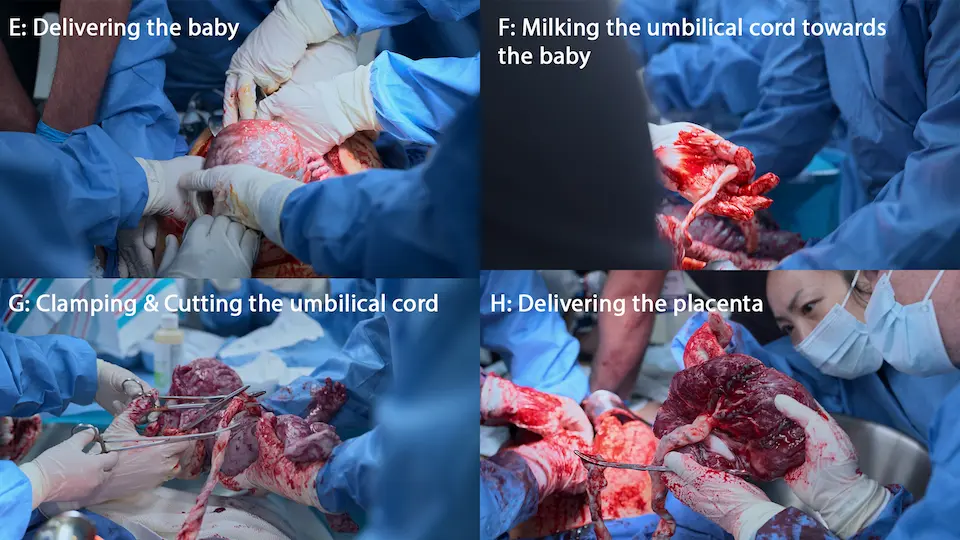
- Delivery of infant
- Delivery of placenta
- 10 units IV Pitocin & Uterine massage
⮑ Outcome & Reassessment
Infant delivered successfully. Mother remains in arrest, transitioning from V-Fib to PEA.
Clinical Media


Neonatal Resuscitation & Ongoing Maternal ACLS
Delivery of compromised, apneic neonate
+1
Neonatal Resuscitation & Ongoing Maternal ACLS
Delivery of compromised, apneic neonate
Medical Decision Making
Neonate is apneic and bradycardic (HR < 100 bpm). Needs immediate stimulation, suction, and positive pressure ventilation (PPV). Pulse ox targets for a newborn rise slowly; a SpO2 in the 60s at 1 minute is physiologically normal, avoiding the need for immediate intubation based purely on SpO2. Meanwhile, maternal ACLS must continue uninterrupted.
Diagnostics & Findings
- Neonatal APGAR scoring (1 min and 5 min)
- Maternal rhythm and pulse checks
Findings:
- Neonate 1 min APGAR: 5 (0 for color, 2 for HR, 1 for reflex, tone, breathing)
- Maternal V-Fib persists
Interventions
- Neonatal suction (DeLee trap) and blow-by oxygen / Bagging
- Maternal defibrillation
- Maternal chest compressions resumed
⮑ Outcome & Reassessment
Neonatal HR begins climbing. Maternal V-Fib converted into a different rhythm on the next pulse check.
Clinical Media

Rhythm Check & Hemorrhage Control
Scheduled ACLS rhythm check; ongoing massive uterine hemorrhage
+2
Rhythm Check & Hemorrhage Control
Scheduled ACLS rhythm check; ongoing massive uterine hemorrhage
Medical Decision Making
Monitor displays organized sinus rhythm but no carotid pulse is palpable, indicating Pulseless Electrical Activity (PEA). CPR must be immediately resumed. The primary reversible cause (the 'H' in H's and T's) is profound hypovolemia secondary to the coagulopathy of HELLP syndrome and the surgical incision. Immediate aggressive mechanical hemostasis (laparotomy pad packing) and continued mass transfusion are necessary to restore intravascular volume and achieve ROSC.
Diagnostics & Findings
- Rhythm and pulse check
Findings:
- Organized electrical rhythm (Sinus)
- Absent carotid pulse (PEA)
- Profuse, ongoing uterine bleeding
Interventions
- Resume chest compressions
- Transfuse additional 2 units of uncrossmatched blood
- Pack the open uterus with laparotomy (lap) pads for direct pressure hemostasis
⮑ Outcome & Reassessment
PEA continues; CPR ongoing while massive transfusion catches up with volume loss. Uterine bleeding is managed with direct pressure.
Clinical Media


Maternal ROSC & Neonatal Stabilization
Subsequent rhythm check and 5-minute neonatal APGAR assessment
Maternal ROSC & Neonatal Stabilization
Subsequent rhythm check and 5-minute neonatal APGAR assessment
Medical Decision Making
With aggressive volume replacement (6 units total) and uterine packing, the maternal cardiovascular system has enough preload to generate a perfusing pulse, achieving ROSC. The neonate has responded well to suction and PPV, improving heart rate and tone, meaning further invasive airway management is not currently needed. Both patients are stabilized enough for definitive transfer.
Diagnostics & Findings
- Maternal pulse and rhythm check
- Maternal Hemoglobin reassessment
- Neonatal 5-minute APGAR scoring
Findings:
- Maternal: Palpable weak carotid pulse, Sinus Rhythm
- Maternal: Hemoglobin risen to 9 g/dL
- Maternal: EEG shows no seizure activity
- Neonate: 5-minute APGAR of 8 (normal SpO2 at 5 min is 80%)
Interventions
- Halt CPR
- Cycle blood pressure cuff
- Transfer protocols initiated for OR (Mother) and NICU (Neonate)
⮑ Outcome & Reassessment
Maternal ROSC sustained; bleeding slowed to an ooze. Neonatal HR normalizes to 132 bpm. Massive success.
Diagnoses & Disposition
Evolving Diagnoses
- [Pre-hospital]Severe Preeclampsia
- [ED Trauma Bay]Eclampsia
- [ED Trauma Bay]HELLP Syndrome (Hemolysis, Elevated Liver enzymes, Low Platelets)
- [ED Trauma Bay]Refractory Non-Convulsive Status Epilepticus
- [ED Trauma Bay]Maternal Cardiac Arrest (V-Fib / PEA)
Current Disposition
Maternal ROSC achieved; patient transferred to the Operating Room with Obstetrics. Neonate successfully resuscitated and transferred to the NICU.
Casebook Analysis
Episode Context
The case highlights the extreme dangers of completely unmanaged 'wild pregnancies.' The narrative forces the ED team already stretched thin and dealing with internal interpersonal drama to perfectly execute one of the most high-stakes, time-sensitive procedures in emergency medicine: the perimortem C-section. It serves as a triumphant unifying moment for the ED team.
Attending's Review
Medical Accuracy
The episode displays incredible medical accuracy. The rationale for choosing Succinylcholine over Rocuronium during RSI for a status epilepticus patient is a fantastic, highly advanced clinical pearl accurately represented here. Left Uterine Displacement (LUD) during CPR is correctly instituted. Utilizing Ketamine for refractory status epilepticus reflects modern, progressive critical care guidelines. The APGAR scoring debate correctly identifies that neonatal SpO2 normally takes up to 10 minutes to reach >90%.
Complications & Errors
- TV Timing: The resuscitative hysterotomy is stated to have taken '36 seconds.' While the initial incision and delivery can be incredibly fast (usually aiming for under 1 minute), achieving hemostasis and surviving this procedure with a platelet count of 40,000 without immediate catastrophic exsanguination is highly dramatized.
- Maternal ROSC Timeline: Obtaining sustained maternal ROSC almost immediately after delivery, while actively hemorrhaging from a massive laparotomy in the setting of severe HELLP syndrome, represents an incredibly unlikely best-case scenario.
Clinical Pearls
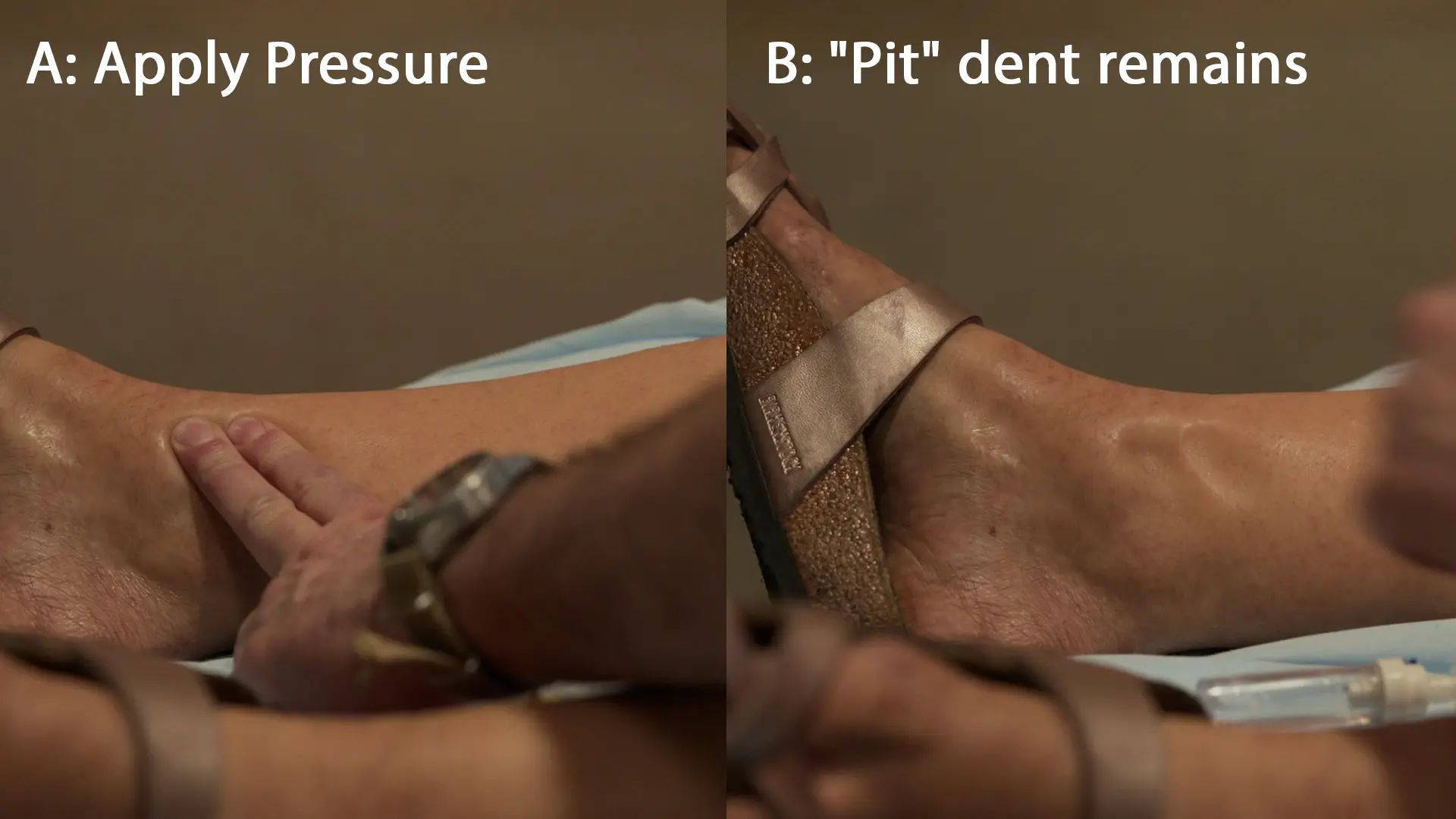
Pathophysiology of Edema in Preeclampsia: Preeclampsia induces widespread maternal endothelial dysfunction, leading to increased capillary permeability. Combined with protein loss in the urine (which reduces serum oncotic pressure), fluid third-spaces into the interstitial compartment. When pressure is applied during a physical exam, the interstitial fluid is mechanically displaced, leaving a classic 'pit' that slowly refills as fluid returns.
Cardiotocography (CTG) utilizes two transducers: a tocodynamometer placed over the uterine fundus to measure contraction frequency, and an ultrasound transducer placed lower over the fetal back to continuously monitor the fetal heart rate. The mother is placed with a slight lateral tilt (left uterine displacement) to prevent the gravid uterus from compressing the inferior vena cava, ensuring adequate venous return to the heart and optimal placental perfusion.
The Dangers of 'Wild Pregnancies': The patient's desire for a 'free birth' without medical intervention ignores critical screening for conditions like preeclampsia. Dr. Abbot accurately cites that historical, unassisted childbirth carried an infant mortality rate of roughly 30%. While modern sanitation and nutrition have improved baseline survival, pregnant individuals receiving no prenatal care today still face a 3 to 4 times higher risk of pregnancy-related maternal death and a significantly increased risk of stillbirth, neonatal death, and severe morbidities such as eclampsia and HELLP syndrome.
HELLP Syndrome: Hemolysis, Elevated Liver enzymes, and Low Platelets characterize this severe, life-threatening complication of preeclampsia. Driven by microangiopathic endothelial damage and microvascular thrombosis, it results in rapid platelet consumption and hepatic ischemia. Delivery of the fetus is the only definitive cure. In the ED, it necessitates extreme vigilance for spontaneous hemorrhage, seizure prophylaxis (Magnesium Sulfate), tight blood pressure control, and preparation for massive transfusion protocols if surgical intervention is needed.
Preeclampsia to Eclampsia Transition: The defining event that upgrades severe preeclampsia to eclampsia is the occurrence of new-onset, generalized tonic-clonic seizures. This transition is driven by severe cerebral vasospasm, endothelial dysfunction, and a breakdown of the blood-brain barrier resulting in cerebral edema. Severe, unrelenting headaches and visual disturbances (as seen in this patient) are classic warning signs of impending eclampsia. While intravenous Magnesium Sulfate is the first-line agent to raise the seizure threshold and prevent this transition, breakthrough seizures require immediate airway protection, secondary anti-epileptic drugs, and expedited delivery of the fetus as the definitive treatment.
RSI Pharmacology in Status Epilepticus: When performing Rapid Sequence Intubation (RSI) on a seizing patient, the choice of medications is critical. Dr. Abbot correctly selects Propofol and Succinylcholine over Etomidate and Rocuronium. Propofol provides intrinsic anti-seizure properties via GABA-receptor agonism, helping to terminate the cerebral electrical storm. Succinylcholine is a short-acting paralytic (~5-10 minutes); using it instead of a long-acting agent like Rocuronium prevents prolonged masking of motor seizure activity, allowing the team to quickly perform a clinical neuro exam to check for non-convulsive status epilepticus once the blockade wears off.
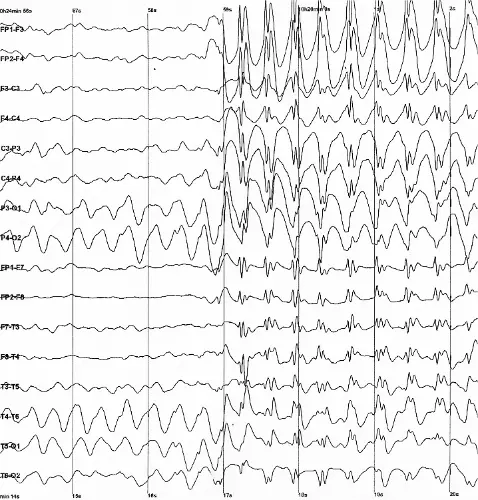
Refractory Status Epilepticus in Eclampsia: Status epilepticus (SE) is defined as continuous seizure activity lasting ≥5 minutes or recurrent seizures without a return to baseline. On an EEG, it classically presents as continuous, high-amplitude 'spike-and-wave' discharges, where the spike represents synchronous neuronal depolarization and the wave represents subsequent inhibition. While classic eclamptic seizures are usually brief and self-limiting, this patient progressed into non-convulsive status epilepticus (confirmed via EEG after neuromuscular blockade). This is a life-threatening obstetric emergency indicating severe cerebral edema and ischemia. It mandates immediate escalation past standard magnesium therapy to aggressive anesthetics (like Ketamine and Propofol) and emergent delivery of the fetus, as removing the placenta is the only definitive way to halt the underlying cascade.
The 4-Minute Rule: In maternal cardiac arrest with a viable fetus (>24 weeks), if ROSC is not achieved within 4 minutes, a resuscitative hysterotomy must be initiated to deliver the fetus by minute 5. This is primarily a resuscitative procedure for the mother to relieve aortocaval compression.
Resuscitative Hysterotomy vs. Perimortem C-Section: Modern emergency medicine and obstetrics have shifted away from the term 'perimortem C-section' in favor of 'resuscitative hysterotomy.' The older term falsely implied the procedure was a last-ditch effort solely for fetal salvage after maternal death was certain. The new terminology correctly frames the procedure as a critical, active resuscitative intervention for the mother. Emptying the gravid uterus immediately relieves aortocaval compression, drastically increasing venous return to the heart and improving the efficacy of CPR, thereby maximizing the chances of maternal Return of Spontaneous Circulation (ROSC).
Left Uterine Displacement: During maternal CPR, manual leftward displacement of the uterus (or tilting the patient 15-30 degrees to the left) is critical to relieve pressure on the inferior vena cava and optimize venous return.
Targeted Neonatal Oxygenation: Newborns naturally have low oxygen saturations immediately after birth. A SpO2 in the 60% range at 1 minute of life is considered physiologically normal; aggressive hyperoxygenation should be avoided.
Neonatal Resuscitation Algorithm (HR < 100 bpm): According to NRP guidelines, if a newly delivered infant is apneic, gasping, or has a heart rate less than 100 bpm, immediate intervention is required. The first steps involve warming, drying, and stimulating the infant while positioning the airway (the 'sniffing' position). If secretions are present, the airway must be cleared using a bulb syringe or suction catheter. The crucial rule is to suction the 'Mouth before Nose' (M before N); suctioning the nose first can trigger a reflex gasp, causing the neonate to aspirate oral secretions. If the heart rate remains below 100 bpm after initial stimulation and airway clearance, the provider must immediately initiate Positive Pressure Ventilation (PPV) via bag-valve-mask at a rate of 40-60 breaths per minute, which is the most critical and effective step in neonatal resuscitation.
Similar Cases from The Show


Chart Navigation
Judith Lastrade
C/O10/10 headache and blurred vision at 36-37 weeks gestation