History of Present Illness
52-year-old male, chief rigger for a music festival, brought in by EMS after a speaker tower fell on his left side. EMS reports isolated trauma to the left chest with obvious multiple rib fractures. Received 50mcg of Fentanyl in the field.

Emergency Department Course
Triage & Initial Evaluation
EMS Arrival
+1
Triage & Initial Evaluation
EMS Arrival
Medical Decision Making
Patient has significant blunt force thoracic trauma. Primary concern is underlying organ injury, particularly pneumothorax, hemothorax, or splenic laceration. FAST/POCUS is performed immediately to rule out free fluid in the abdomen and gross hemopneumothorax. Given the patient's desire to remain awake to manage his festival crew, regional anesthesia is preferred over systemic narcotics to prevent respiratory depression.
Diagnostics & Findings
- POCUS / FAST exam
- CT Chest/Abdomen/Pelvis with contrast
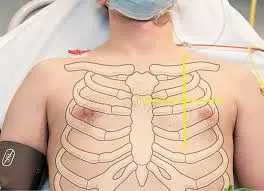
Findings:
- Obvious flail chest on the left
- No hemopneumothorax visualized on initial POCUS
- Benign abdomen with no free fluid on FAST
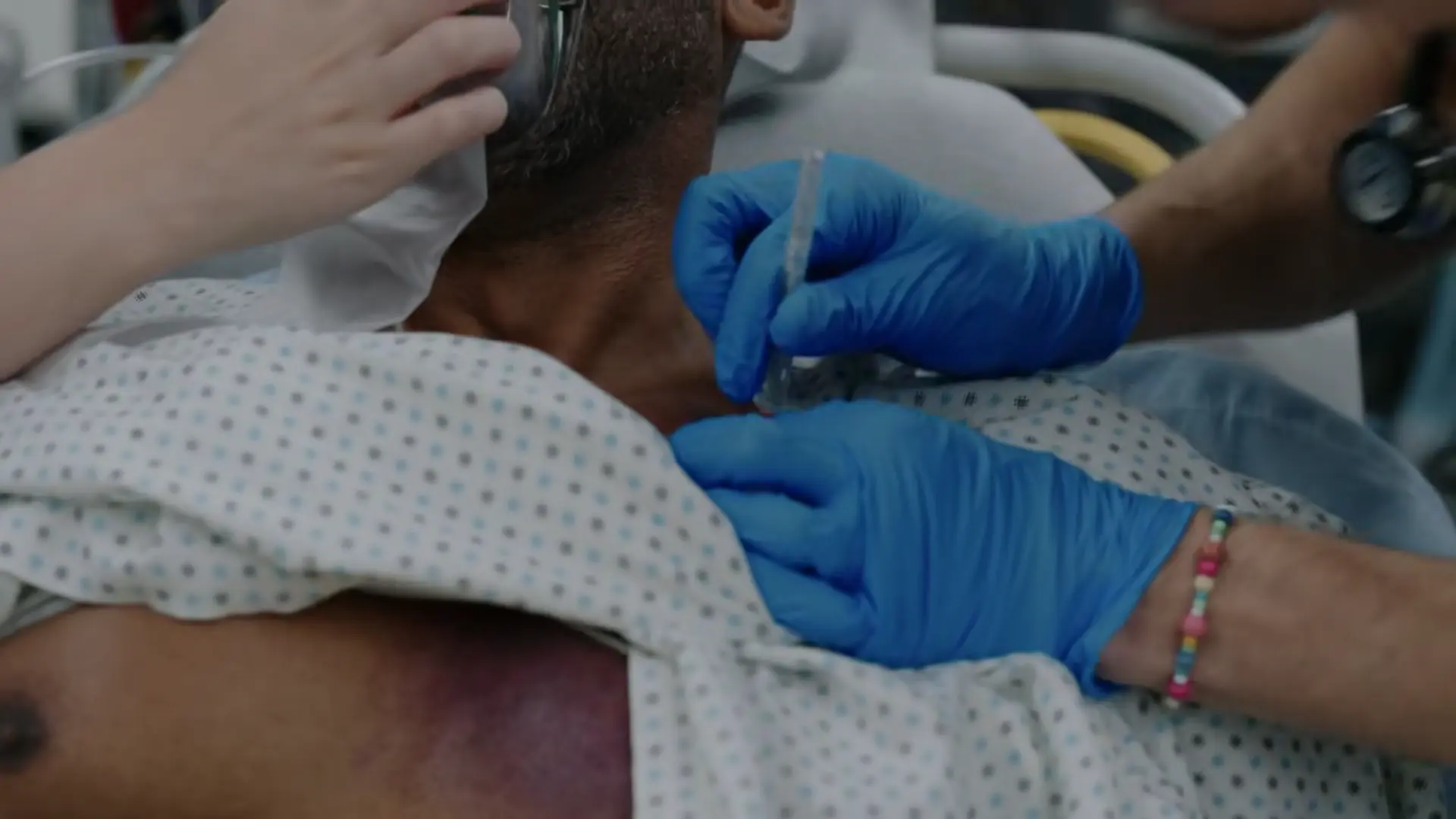
Interventions
- Serratus anterior plane block down to T-9
⮑ Outcome & Reassessment
Patient tolerates the block well. Sent to CT for definitive imaging.
Clinical Media

Reassessment & Independent Intervention
Post-CT Status Update & Hypoxia
Reassessment & Independent Intervention
Post-CT Status Update & Hypoxia
Medical Decision Making
CT revealed a small pneumothorax and underlying pulmonary contusions. The regional block successfully eliminated the patient's pain. However, his oxygen saturations are dropping due to V/Q mismatch from the bruised lung. Santos independently decides to initiate Non-Invasive Positive Pressure Ventilation (BiPAP) to recruit alveoli and improve oxygenation, failing to recognize the absolute contraindication of applying positive pressure to an untreated pneumothorax.
Diagnostics & Findings
- Review of CT results
Findings:
- Small pneumothorax
- Lung contusions
Interventions
- Initiated BiPAP 10/5
⮑ Outcome & Reassessment
Pain remains well-controlled, but BiPAP setup precipitates a life-threatening complication moments later.
Code/Crash
Rapid clinical deterioration and monitor alarms
+3
Code/Crash
Rapid clinical deterioration and monitor alarms
Medical Decision Making
Patient is in obstructive shock. The positive pressure from the BiPAP forced air into the pleural space through the visceral pleural tear, creating a one-way valve effect. This rapidly expanded the small pneumothorax into a tension pneumothorax, shifting the mediastinum and compressing the superior vena cava, causing hypotension and severe hypoxia. Immediate needle decompression is required to convert the tension pneumothorax back to a simple pneumothorax, followed by a pigtail catheter placement for definitive drainage.
Diagnostics & Findings
- Auscultation
- Tracheal exam
Findings:
- Absent breath sounds on the left
- Tracheal deviation to the right
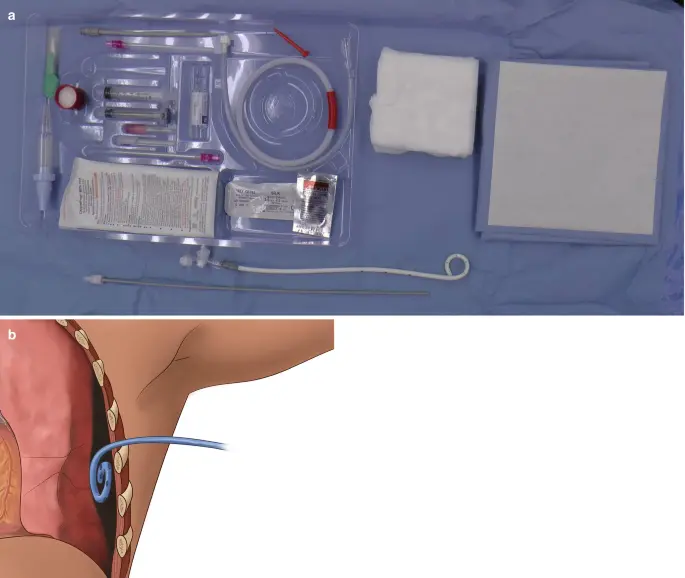
Interventions
- Immediate needle decompression with 14 gauge angiocath
- Switched from BiPAP to Non-Rebreather mask
- Pigtail catheter placement (tube thoracostomy)
- Administered 75mg Ketamine for procedural sedation
⮑ Outcome & Reassessment
Audible hiss heard upon needle decompression. Saturations and blood pressure both improved rapidly.
Clinical Media

Status Check & Transfer of Care
Follow-up post-procedure
+1
Status Check & Transfer of Care
Follow-up post-procedure
Medical Decision Making
Patient is now hemodynamically stable and oxygenating well with the pigtail catheter in place. The injuries (six rib fractures, pulmonary contusion, chest tube) necessitate admission to a higher level of care for observation and continued pain management. Thoracic surgery consultation is appropriate.
Diagnostics & Findings
Findings:
- Vitals normalized
- Six rib fractures confirmed
Interventions
- Consulted Thoracic Surgery (Dr. Gregorian)
⮑ Outcome & Reassessment
Patient is stable, alert, and demanding to return to work. Admitted to Thoracic Surgery.
Clinical Media
Diagnoses & Disposition
Evolving Diagnoses
- [Triage]Multiple left rib fractures with flail chest
- [Post-CT]Small left pneumothorax and pulmonary contusion
- [Crash]Iatrogenic Tension Pneumothorax
Current Disposition
Admitted to Thoracic Surgery (Dr. Gregorian) for observation and management of rib fractures and pigtail catheter.
Casebook Analysis
Episode Context
Wendell serves as the high-stakes, fast-paced trauma case of the episode. His clinical arc is primarily utilized to demonstrate the dangers of premature decision-making by inexperienced residents (Dr. Santos), highlighting the rigid hierarchy and necessary supervision protocols within emergency medicine training.
Attending's Review
Medical Accuracy
The medicine in this sequence is highly accurate and represents a classic EM teaching scenario. Using a Serratus Anterior Plane block for rib fractures is a modern, excellent standard of care that avoids respiratory depression. The iatrogenic tension pneumothorax caused by applying positive pressure (BiPAP) to an untreated small pneumothorax is a textbook medical error. Dr. Langdon's correction to use a pigtail catheter instead of a traditional large-bore surgical chest tube for a simple pneumothorax reflects current, less-invasive ATLS/trauma guidelines.
Complications & Errors
- Iatrogenic Tension Pneumothorax: Dr. Santos ordered BiPAP to treat hypoxia caused by lung contusions, failing to realize that positive pressure ventilation would rapidly expand the patient's existing, small pneumothorax.
Clinical Pearls
Never apply non-invasive positive pressure ventilation (BiPAP/CPAP) to a patient with an untreated pneumothorax unless a chest tube is placed, as it acts as a one-way valve and will precipitate a tension pneumothorax.
Serratus anterior plane blocks provide excellent regional analgesia for multiple rib fractures, avoiding the respiratory depressant effects of systemic opioids, which is crucial in trauma patients with pulmonary contusions.
When deciding between a small-bore pigtail catheter and a traditional large-bore chest tube (tube thoracostomy), consider the substance being drained. Pigtail catheters (≤14 French) are the modern standard of care for isolated pneumothoraces (air), as they are equally effective, less invasive, and significantly less painful. Large-bore chest tubes (≥24 French) are typically reserved for draining thick fluids, such as blood in a hemothorax or pus in an empyema, which would otherwise occlude a small-bore catheter.
Similar Cases from The Show



Chart Navigation
Wendell Stone
C/OIsolated left chest trauma from a crush injury.