History of Present Illness
Alex is a young adult male who presented to the ED ambulance bay as a 'drop-off' from a private vehicle. He complains of severe abdominal pain secondary to a gunshot wound (GSW). He has no known daily medications and no known allergies.

Emergency Department Course
Trauma Resuscitation & Diagnostic Imaging
Patient dumped at ambulance bay with a penetrating abdominal injury.
+1
Trauma Resuscitation & Diagnostic Imaging
Patient dumped at ambulance bay with a penetrating abdominal injury.
Medical Decision Making
Patient is in hemorrhagic shock (systolic 80) from a penetrating abdominal injury. Immediate priorities are securing large-bore IV access, initiating volume expansion with blood products (not crystalloids) via rapid infuser, prophylactic antibiotics, and a FAST exam to identify the source of intraperitoneal bleeding before emergent surgical source control.
Diagnostics & Findings
- Primary Survey
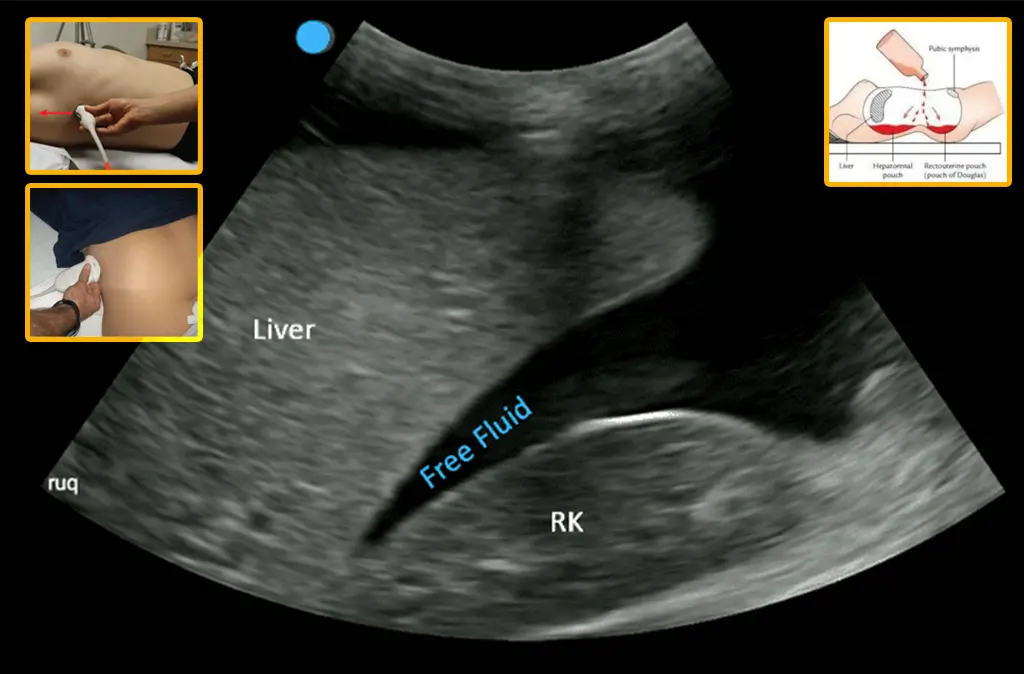
- FAST Exam (Focused Assessment with Sonography for Trauma)
Findings:
- Lungs are 'up' (bilateral breath sounds present, ruling out pneumo/hemothorax).
- FAST exam positive: Morrison's pouch is full of blood, indicating a severe liver laceration.
Interventions
- Placed 14-gauge IV in the left antecubital (AC) fossa.
- Initiated 2 units of whole blood via rapid infuser.
- Consulted OR for immediate exploratory laparotomy.
⮑ Outcome & Reassessment
Blood pressure began to rise ('coming up a bit') following the initiation of whole blood. Patient remained alert enough to request his mother be called ('ICE' on his cell phone). Transported emergently to the OR.
Clinical Media
Diagnoses & Disposition
Evolving Diagnoses
- [S01E02]Abdominal Gunshot Wound
- [S01E02]Hemorrhagic Shock
- [S01E02]Grade IV/V Liver Laceration
Current Disposition
Transferred emergently to the Operating Room (OR).
Casebook Analysis
Episode Context
Alex's case serves as a high-octane trauma insertion to showcase the capabilities and readiness of a Level 1 Trauma Center. It creates a teaching moment highlighting that the hospital always keeps an OR fully stocked and prepped for zero-notice emergencies.
Attending's Review
Medical Accuracy
The trauma resuscitation is depicted with high clinical fidelity. The use of a 14-gauge IV (standard for rapid fluid/blood administration), initiating whole blood on a rapid infuser for a hypotensive patient (systolic 80) are textbook trauma protocols. Performing a FAST exam to identify fluid in Morrison's pouch (the hepatorenal recess) correctly diagnoses the bleeding liver, prompting immediate transport to the OR. The cross-talk regarding Orthopedics accurately reflects the chaotic nature of a busy trauma bay where multiple critical cases are being managed simultaneously by the surgical team.
Clinical Pearls
The ATLS Primary Survey follows the ABCDE protocol (Airway, Breathing, Circulation, Disability, Exposure). In this case, Airway and Disability were intact as the patient was speaking and alert (GCS 15). Breathing was confirmed adequate ('Lungs up'). The team correctly recognized the immediate life threat and heavily focused on Circulation, treating profound hemorrhagic shock (systolic 80) with a large-bore IV, rapid whole blood transfusion, and a FAST exam to identify the intra-abdominal bleeding source.
The FAST (Focused Assessment with Sonography for Trauma) exam is a rapid bedside ultrasound designed to identify life-threatening free fluid (blood) in four dependent anatomical regions: 1) Cardiac (subxiphoid) for pericardial effusion, 2) Right Upper Quadrant (RUQ), evaluating the hepatorenal recess known as Morrison's Pouch, 3) Left Upper Quadrant (LUQ), evaluating the splenorenal recess, and 4) Pelvic (suprapubic), evaluating the rectovesical/rectouterine space. In this patient, a positive FAST in Morrison's Pouch confirmed massive intraperitoneal hemorrhage.
In penetrating abdominal trauma with hemodynamic instability, the definitive treatment is surgical source control (exploratory laparotomy). Time spent in the ED should be minimized.
Resuscitation of hemorrhagic shock prioritizes balanced blood products or whole blood over crystalloids (like normal saline) to prevent dilutional coagulopathy and maintain oxygen-carrying capacity.
Level 1 Trauma Centers operate under strict American College of Surgeons (ACS) guidelines requiring a dedicated operating room to be staffed and immediately available 24/7. This 'always ready' posture extends to other critical interventions, including storing uncrossmatched O-type blood (or low-titer O+ whole blood) in ED coolers for immediate Massive Transfusion Protocol (MTP) initiation, maintaining primed rapid infusers, and requiring in-house trauma surgery and anesthesia teams.


