History of Present Illness
79-year-old male from an assisted living facility presenting to the ED with a fever and cough. He has a history of mild Alzheimer's disease. On arrival, he is tachycardic, hypotensive, and experiencing altered mental status (asking if it is dinnertime). A POLST form from his facility indicates he is to receive IV fluids and medications, but no intubation and no chest compressions (DNI/No CPR).

Emergency Department Course
Initial Evaluation & Intervention
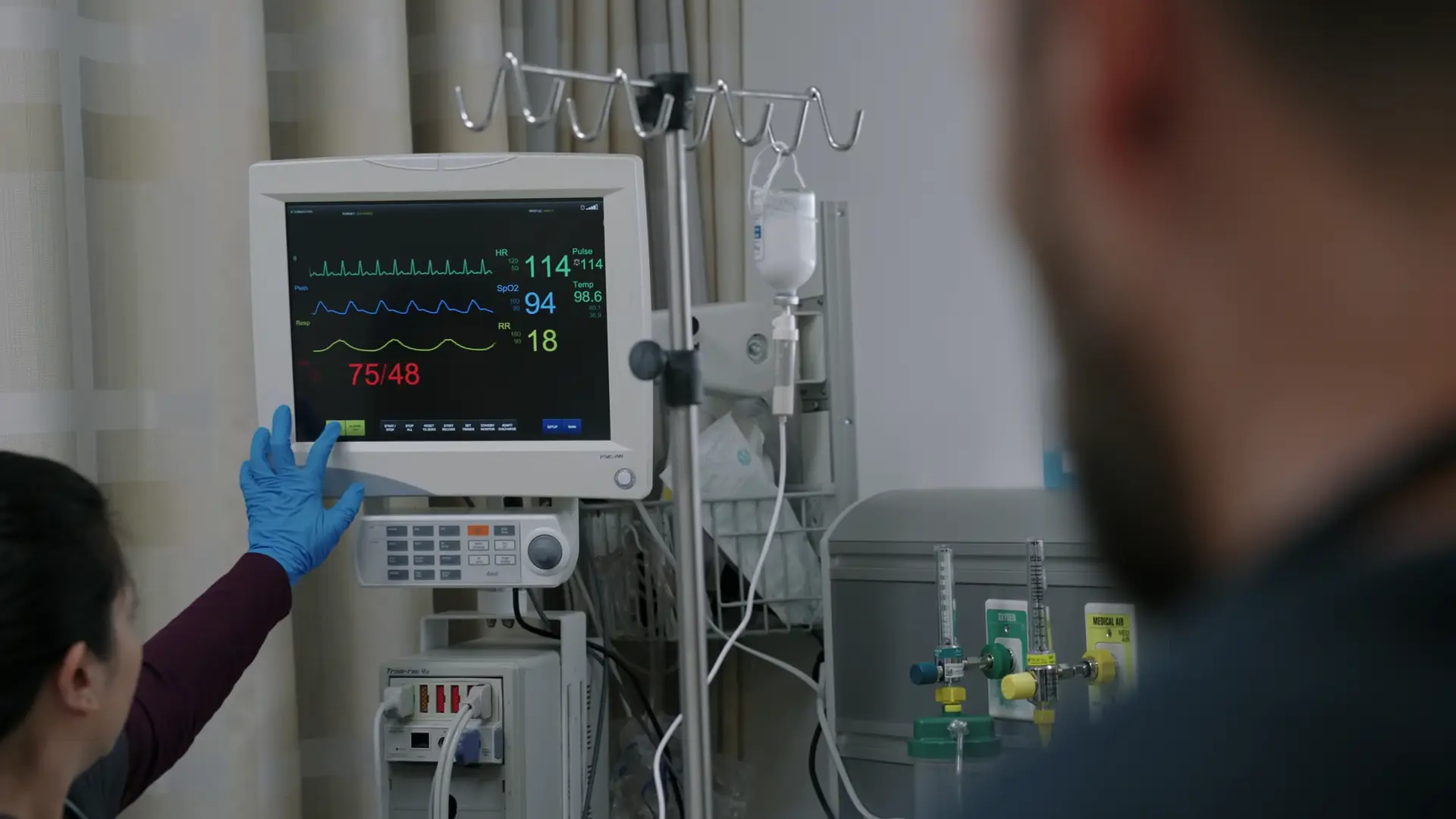
Patient arrival from an assisted living facility demonstrating signs of systemic inflammatory response syndrome (SIRS) and hypoperfusion.
Initial Evaluation & Intervention
Patient arrival from an assisted living facility demonstrating signs of systemic inflammatory response syndrome (SIRS) and hypoperfusion.
Medical Decision Making
The patient is an elderly male with fever, cough, tachycardia, and hypotension. Lung auscultation reveals coarse rhonchi, and imaging shows a right middle lobe infiltrate. This constellation of signs clearly indicates sepsis secondary to pneumonia. A 'Code Sepsis' is initiated to ensure rapid compliance with CMS guidelines (SEP-1 core measure bundle), which requires measuring a lactate level, obtaining blood cultures prior to administering broad-spectrum antibiotics, and administering a 30 cc/kg crystalloid fluid bolus for hypotension.
Diagnostics & Findings
- Lung auscultation
- Chest X-ray (revealing RML infiltrate)
- Two sets of blood cultures ordered
- Lactic acid ordered
Findings:
- Coarse rhonchi on auscultation
- Right middle lobe infiltrate
- Fever of 102.0 F
- Altered mental status/Confusion
Interventions
- Review of POLST (DNI/No CPR confirmed)
- Initial 500 cc normal saline bolus
- 30 cc/kg normal saline ordered
- Ceftriaxone 1g IV ordered
- Azithromycin 500mg IV ordered
⮑ Outcome & Reassessment
Patient remains confused but compliant. Treatment protocol initiated pending lab results and response to fluid resuscitation.
Status Update & Goals of Care Discussion
Family (son and daughter) arrives and requests an update on their father's condition.
Status Update & Goals of Care Discussion
Family (son and daughter) arrives and requests an update on their father's condition.
Medical Decision Making
The patient's blood pressure is improving following the sepsis fluid resuscitation, but he continues to experience significant delirium (calling out random words and names). Because the patient has a documented DNI (Do Not Intubate) and DNR (Do Not Resuscitate) in his advanced directive, it is crucial to establish clear goals of care with the family members who hold Durable Power of Attorney for Healthcare, preparing them for potential respiratory decline.
Diagnostics & Findings
Findings:
- Improving hemodynamics (BP increasing)
- Persistent altered mental status / delirium
Interventions
- Family conference regarding prognosis and advanced directives
- Continued IV fluids, antibiotics, and supplemental oxygen
⮑ Outcome & Reassessment
Patient remains delirious, quoting 'Nowhere Man'. Family is hesitant to accept the DNI directive, requesting time to think about allowing a natural death versus intervening if he worsens.
Clinical Deterioration
Oxygen saturation alarms trigger indicating acute hypoxia.
+1
Clinical Deterioration
Oxygen saturation alarms trigger indicating acute hypoxia.
Medical Decision Making
The patient is acutely desaturating and exhibiting worsening confusion. The differential for this acute decompensation includes progression of his pneumonia or, highly likely in this elderly patient, iatrogenic pulmonary edema secondary to the aggressive 30cc/kg fluid bolus required for his earlier sepsis/hypotension. Diuresis (removing fluid) is contraindicated because his blood pressure would crash back into septic shock. To support his oxygenation without violating his written DNI order, non-invasive positive pressure ventilation (BiPAP) is the most appropriate step.
Diagnostics & Findings
- Continuous pulse oximetry monitoring
Findings:
- Acute hypoxia
- Worsening confusion ('I don't remember where I parked')
Interventions
- Initiated BiPAP at 15/5 cmH2O
⮑ Outcome & Reassessment
Patient placed on BiPAP. Dr. Robby warns the family that if BiPAP fails, a definitive decision on intubation (against his advanced directive) must be made.
Clinical Media

Critical Deterioration & Ethical Conflict
Patient failing maximal non-invasive ventilation (BiPAP maxed out).
Critical Deterioration & Ethical Conflict
Patient failing maximal non-invasive ventilation (BiPAP maxed out).
Medical Decision Making
The patient has reached maximum settings on BiPAP (25/10) and remains profoundly hypoxic (SpO2 in the high 80s). Medically, he requires immediate endotracheal intubation. However, ethically and legally, there is a conflict: the patient has a written DNI, but the family (acting as Durable Power of Attorney for Healthcare) is aggressively demanding intubation and threatening hospital legal action if their proxy demand is not met. Without time to consult the hospital Ethics Committee due to the patient's imminent respiratory collapse, Dr. Robby is forced into a corner to comply with the DPOA's demands to intubate.
Diagnostics & Findings
- Pulse oximetry evaluation on max BiPAP
Findings:
- BiPAP failure (settings 25/10)
- Refractory hypoxia (High 80s)
Interventions
- Decision made to proceed with Endotracheal Intubation (overriding written DNI per DPOA demand)
⮑ Outcome & Reassessment
Preparation for emergent intubation is underway as the family refuses to allow a natural death.
Sedation Adjustment & Restraint Application
Patient agitation and attempt to self-extubate.
Sedation Adjustment & Restraint Application
Patient agitation and attempt to self-extubate.
Medical Decision Making
Following the forced intubation against his DNI advanced directive in Episode 2, the patient is boarding in the ED and experiencing significant distress and delirium while on the mechanical ventilator. He attempts to pull out his endotracheal (ET) tube. To prevent a traumatic, unplanned extubation, the clinical team must increase chemical sedation (propofol infusion) and rely on physical soft restraints.
Diagnostics & Findings
- Clinical observation of agitation and ventilator dyssynchrony
Findings:
- Attempted self-extubation
- Agitation/Delirium
Interventions
- Application of bilateral soft physical restraints
- Increased Propofol continuous IV infusion
⮑ Outcome & Reassessment
Patient physically restrained; sedation deepened to achieve appropriate RASS (Richmond Agitation-Sedation Scale) goal and ensure ET tube safety while boarding in the ED.
Hemodynamic Collapse & Goals of Care
Patient experiences dropping blood pressure and worsening hypoxia while agitated on the ventilator. Family is distressed by his suffering.
+2
Hemodynamic Collapse & Goals of Care
Patient experiences dropping blood pressure and worsening hypoxia while agitated on the ventilator. Family is distressed by his suffering.
Medical Decision Making
The patient is developing septic shock. Dr. Robby correctly identifies that standard fluid resuscitation is absolutely contraindicated due to his existing iatrogenic pulmonary edema (fluids will 'just fill up his lungs'). The next indicated step for fluid-refractory shock is initiating a vasopressor (Levophed/norepinephrine) via a central venous catheter ('long, large IV catheter in his jugular vein'). However, Dr. Robby frames this medically indicated step within the ethical context of the patient's terminal prognosis, explaining to the family that escalating to a central line and pressors will likely cause ischemic organ damage and prolong suffering without meaningful clinical benefit.
Diagnostics & Findings
- Continuous hemodynamic monitoring
- Ventilator assessment (100% FiO2)
Findings:
- Refractory hypotension
- Refractory hypoxia despite 100% O2
- Agitation/Delirium
Interventions
- Family counseling on the risks vs. benefits of a Central Venous Catheter and Levophed
- Recommendation to halt further invasive escalation
⮑ Outcome & Reassessment
The family begins to realize the futility of aggressive measures as the patient continues to fail on the ventilator and slide into shock.
Clinical Media

Palliative Care & Terminal Extubation
Family grappling with the reality of their father's terminal decline and active suffering on the ventilator.
Palliative Care & Terminal Extubation
Family grappling with the reality of their father's terminal decline and active suffering on the ventilator.
Medical Decision Making
With the patient failing mechanical ventilation and developing refractory shock, continuing aggressive care explicitly violates his original DNI/DNR wishes and is actively prolonging the dying process. Dr. Robby proposes 'compassionate extubation' (palliative extubation). By removing the endotracheal tube and weaning sedation, the patient may briefly regain consciousness to interact with his family, while supplemental oxygen ensures he passes peacefully without the discomfort of the tube.
Diagnostics & Findings
Findings:
- Irreversible multiorgan failure
- Family acceptance of terminal prognosis
Interventions
- Initiated Comfort Measures Only (CMO) discussion
- Decision finalized to perform palliative extubation
⮑ Outcome & Reassessment
The family agrees to the humane, palliative approach, resolving the ethical conflict from the prior episode by prioritizing the patient's comfort and peaceful passing.
Diagnoses & Disposition
Evolving Diagnoses
- [S01E01]Right Middle Lobe Pneumonia
- [S01E01]Sepsis
- [S01E02]Pulmonary Edema (Secondary to fluid resuscitation)
- [S01E02]Acute Hypoxic Respiratory Failure
- [S01E03]Ventilator-associated agitation / Delirium
- [S01E03]Septic Shock (Fluid-refractory hypotension)
- [S01E03]Terminal Extubation / Comfort Measures Only
Current Disposition
Transitioning to Comfort Care / Palliative Extubation to allow a natural, peaceful passing.
Casebook Analysis
Episode Context
The case showcases the ED's morning rush of elderly patients arriving from nursing homes and assisted living facilities. It highlights the systematic nature of handling critical infections ('Code Sepsis') and sheds light on the bureaucratic pressure hospitals face regarding federal audits on sepsis bundle performance metrics. In Episode 2, the case evolves into a profound medical ethics storyline, highlighting the agonizing dilemma when family members with Durable Power of Attorney (DPOA) conflict with a patient's explicitly written advanced directive (DNI/DNR). In Episode 3, the ethical tragedy deepens as Mr. Spencer is shown mechanically ventilated in the ED, agitated, and actively trying to pull out his endotracheal tube. The arc finally concludes when the clinical reality of his multiorgan failure forces the family to recognize his suffering, guiding them toward a compassionate palliative extubation.
Attending's Review
Medical Accuracy
The depiction of the 'Code Sepsis' protocol is highly accurate to modern emergency medicine standards. Drawing blood cultures before administering antibiotics, checking a lactic acid level, ordering 30 cc/kg of crystalloid for hypotension, and using Ceftriaxone plus Azithromycin to cover community-acquired or healthcare-associated pneumonia are all textbook, standard-of-care steps in the CMS SEP-1 core measure. In Episode 2, the development of pulmonary edema after aggressive fluid resuscitation (30cc/kg) for sepsis in an elderly patient is a very common and realistic complication. The ethical conflict regarding DPOA overriding a POLST/Advanced Directive is clinically accurate but legally murky. The events in Episode 3 are exceptionally realistic: Dr. Robby correctly identifies that administering further IV fluids for hypotension would exacerbate the pulmonary edema, necessitating a central line and Levophed (norepinephrine). His honest warning about the ischemic risks ('other organ damage') of high-dose vasopressors in a futile scenario is a hallmark of excellent end-of-life care discussions. The subsequent shift to a 'compassionate extubation' (terminal weaning) with supplemental oxygen for comfort is perfectly aligned with standard palliative care protocols.
Complications & Errors
- Iatrogenic Pulmonary Edema: The patient's lungs filled with fluid as a direct complication of the aggressive fluid resuscitation required for his initial sepsis presentation.
Clinical Pearls
Always check POLST/advanced directives early for patients arriving from assisted living or nursing homes before initiating invasive, life-sustaining procedures.
The 3-hour sepsis bundle requires lactate measurement, blood cultures prior to antibiotics, broad-spectrum antibiotics, and a 30 mL/kg crystalloid bolus for hypotension or a lactate >= 4 mmol/L.
Elderly patients with pneumonia often present with atypical symptoms, such as altered mental status or lethargy, which may be more prominent than the classic respiratory symptoms like cough.
Aggressive fluid resuscitation in elderly patients with sepsis carries a high risk of iatrogenic pulmonary edema, requiring careful balancing of hemodynamics versus respiratory status.
A Durable Power of Attorney for Healthcare (DPOA) can sometimes legally override a written advanced directive if the proxy claims it is what the patient would have wanted, creating significant ethical distress for emergency providers.
Patients with baseline dementia or delirium are at extremely high risk for agitation when mechanically ventilated. Providing adequate sedation (e.g., Propofol, Dexmedetomidine) and applying soft physical restraints are often necessary to prevent traumatic self-extubation.
In fluid-refractory shock, or shock where fluids are contraindicated (e.g., pulmonary edema), the next line of therapy is vasopressors (such as Levophed/norepinephrine) administered via a Central Venous Catheter.
Palliative or 'compassionate' extubation involves removing the endotracheal tube, managing distressing symptoms (like air hunger) with opioids or supplemental oxygen, and occasionally decreasing sedation enough to allow the patient a final meaningful interaction with family before passing.


