History of Present Illness
Patient presents to the ED with left-sided flank pain that began at 10:00 p.m. the previous night. He has a history of kidney stones and states this episode feels exactly the same as prior occurrences. He notes his urine is 'a bit darker than normal' but denies fever or gross hematuria. He suspects he is dehydrated.
Emergency Department Course
Initial Evaluation
Patient roomed with acute flank pain.
+1
Initial Evaluation
Patient roomed with acute flank pain.
Medical Decision Making
The classic presentation of unilateral flank pain with a prior history of nephrolithiasis heavily points toward recurrent renal colic. The absence of fever lowers the suspicion for pyelonephritis or an infected stone, which would be a urologic emergency. The plan is to confirm the clinical suspicion with a bedside physical exam (CVA tenderness) and work up the patient using basic labs (Chem-7 to check renal function, Urinalysis for microscopic hematuria/infection) and a bedside ultrasound (POCUS) to look for hydronephrosis without exposing the patient to unnecessary CT radiation. Ketorolac is ordered for immediate pain control.
Diagnostics & Findings
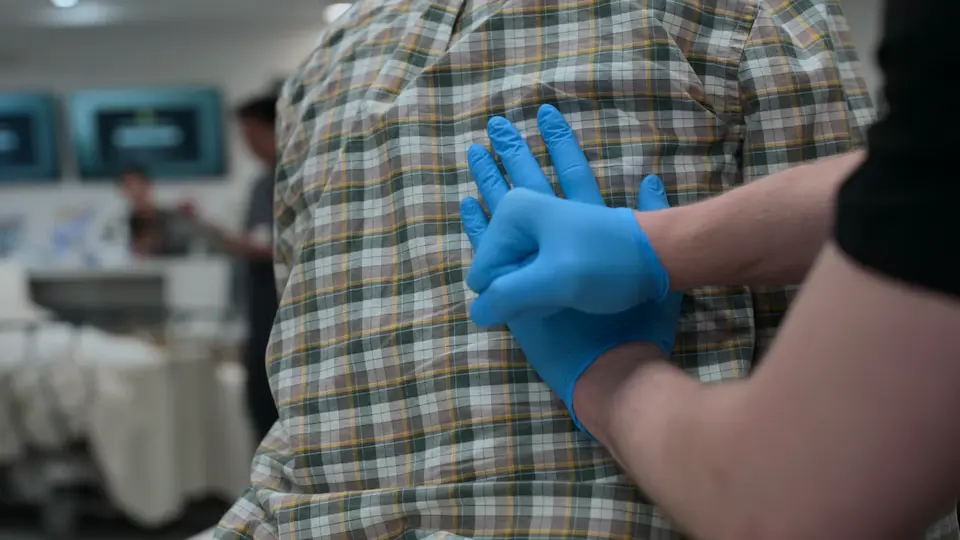
- Costovertebral angle (CVA) percussion
- Urine Dipstick ordered
- Chem-7 ordered
- Bedside Renal Ultrasound ordered
Findings:
- Positive left CVA tenderness on exam
- No fever
Interventions
- Ketorolac 15mg IM ordered
⮑ Outcome & Reassessment
Patient experienced sharp pain upon percussion of the left CVA. Awaiting lab and imaging results.
Clinical Media

Diagnostics Review & Treatment Plan
Return of lab and ultrasound results.
Diagnostics Review & Treatment Plan
Return of lab and ultrasound results.
Medical Decision Making
The urinalysis confirms microscopic hematuria (3+ blood), which is expected as the stone damages the ureteral urothelium. The normal BUN and Creatinine effectively rule out acute kidney injury (AKI); the unaffected right kidney is compensating well. The bedside ultrasound confirms mild hydronephrosis, correlating exactly with the patient's symptoms of a ureteral stone. The pain has responded well to NSAID therapy. Because there are no signs of complicated nephrolithiasis (no AKI, no infection, pain is controllable), the patient can be managed conservatively with continued pain control and observation.
Diagnostics & Findings
Findings:
- Urine dip: 3+ blood
- Chem-7: BUN and Creatinine normal
- Bedside Ultrasound: Mild hydronephrosis consistent with ureteral calculus
Interventions
- Additional Ketorolac 15mg IM ordered
- Continued observation
⮑ Outcome & Reassessment
Patient's pain improved significantly after the first 15mg of Ketorolac IM. Plan is to administer a second dose and continue monitoring.
Status Update & Discharge Delay
Patient is clinically stable but requires final prescriptions and attending sign-off to be formally discharged.
+1
Status Update & Discharge Delay
Patient is clinically stable but requires final prescriptions and attending sign-off to be formally discharged.
Medical Decision Making
The patient's acute pain has been successfully managed, and he is clinically cleared for outpatient management of his uncomplicated renal colic. However, standard ED protocol dictates that the attending physician (Dr. Mohan) must formally sign the discharge orders and finalize any take-home prescriptions (such as oral NSAIDs, antiemetics, or alpha-blockers like tamsulosin). Because Dr. Mohan is currently unavailable due to an acute panic attack / medical episode off-screen, the patient is administratively blocked from leaving. This situation requires holding the patient in the ED until the attending can resume duties or another provider assumes care.
Diagnostics & Findings
Findings:
- Patient is pain-free and clinically stable
- Mentation is intact (demonstrated by grammar pedantry)
Interventions
- Discharge held pending attending signature
- Awaiting pharmacy processing for outpatient prescriptions
⮑ Outcome & Reassessment
Patient is medically stable but increasingly frustrated by the administrative delays. He playfully but strictly maintains his 'English teacher' persona by correcting the staff member's grammar (correcting 'doing good' to 'doing well').
Clinical Media

Status Update
Ongoing delays in processing discharge medications.
Status Update
Ongoing delays in processing discharge medications.
Medical Decision Making
The hospital is experiencing a cyberattack, causing profound delays in pharmacy and overall throughput. The patient remains stable but unable to leave until oral ketorolac prescriptions are dispensed. Continuing to board him in the ED bay while awaiting pharmacy resolution.
Diagnostics & Findings
Findings:
- Patient remains clinically stable, pain-free
Interventions
- Continued observation and follow-up with pharmacy
⮑ Outcome & Reassessment
Patient notes he promised to meet his son at the park for fireworks but remains cooperative while waiting.
Clinical Deterioration
Patient suddenly becomes unresponsive and hypotensive while waiting for discharge.
Clinical Deterioration
Patient suddenly becomes unresponsive and hypotensive while waiting for discharge.
Medical Decision Making
The patient rapidly decompensated with profound hypotension (78/42) and hypoxia (87%). Although a vasovagal episode (secondary to pain) was initially suggested by a staff member, the degree of hypotension and hypoxia without a preceding pain trigger is highly concerning for a true shock state, most likely hemorrhagic given the suddenness. The patient does not even have an IV because he was essentially discharged. He requires immediate transfer to a trauma/resuscitation room for stabilization, access, and diagnostic workup for undifferentiated shock.
Diagnostics & Findings
- Continuous vital sign monitoring
Findings:
- Profound hypotension (78/42)
- Hypoxia (SpO2 87%)
- Altered mental status/unresponsiveness
Interventions
- Immediate transfer to a Trauma Room
⮑ Outcome & Reassessment
Patient is critically ill, hemodynamically unstable, and requires emergent resuscitation.
Diagnosis & Massive Transfusion Protocol (MTP)
Evaluation of undifferentiated shock in a patient previously diagnosed with renal colic.
Diagnosis & Massive Transfusion Protocol (MTP)
Evaluation of undifferentiated shock in a patient previously diagnosed with renal colic.
Medical Decision Making
Dr. Robby identifies the classic cognitive error: hematuria and flank pain in an older male does not always mean a kidney stone; it is also the presentation of an expanding or ruptured Abdominal Aortic Aneurysm (AAA). An immediate E-FAST is performed, revealing an 8-centimeter AAA with massive free fluid (rupture). The patient is exsanguinating. Massive Transfusion Protocol (MTP) is initiated to replace lost volume and oxygen-carrying capacity. Two large-bore peripheral IVs (and a 16-gauge external jugular) are established, emphasizing Poiseuille's law (short, thick catheters provide faster flow than long central lines). The patient is intubated to protect the airway and optimize oxygenation in the setting of severe shock. TXA is given to prevent fibrinolysis. Calcium gluconate is administered proactively to prevent hypocalcemia caused by citrate toxicity from the rapid administration of banked whole blood.
Diagnostics & Findings
- E-FAST (Extended Focused Assessment with Sonography for Trauma)
Findings:
- 8-centimeter Abdominal Aortic Aneurysm (AAA)
- Massive intra-abdominal free fluid (hemorrhage)
Interventions
- Initiated Massive Transfusion Protocol (MTP)
- Placed two large-bore antecubital IVs and one 16-gauge External Jugular (EJ) IV
- Administered 4 units of whole blood via rapid infuser
- Endotracheal intubation (performed by Student Doctor Javadi)
- Administered Tranexamic Acid (TXA) 2 grams
- Administered Calcium Gluconate
- Surgical consultation obtained
⮑ Outcome & Reassessment
Following intubation and the first four units of blood, the patient's blood pressure temporarily improved to 86/52 with a strong radial pulse and good ETCO2 waveform. However, the bleeding rate remains catastrophic.
Cardiac Arrest & Resuscitative Thoracotomy
Patient loses pulses despite aggressive MTP, entering Pulseless Electrical Activity (PEA) arrest.
+3
Cardiac Arrest & Resuscitative Thoracotomy
Patient loses pulses despite aggressive MTP, entering Pulseless Electrical Activity (PEA) arrest.
Medical Decision Making
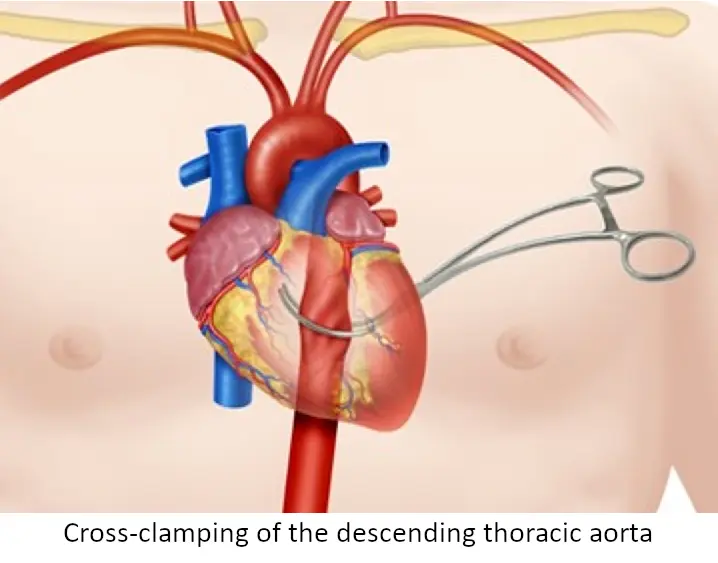
The patient has exsanguinated to the point of cardiac arrest (PEA) because the rate of intra-abdominal bleeding exceeds the rate of MTP resuscitation. The vascular surgeon is delayed. To save the patient's life, the ED team must stop the sub-diaphragmatic blood flow. A resuscitative left anterolateral thoracotomy is indicated to cross-clamp the descending aorta. This 'Hail Mary' procedure will prioritize blood flow to the heart and brain while temporarily halting the catastrophic abdominal hemorrhage, buying time to get the patient to the OR. Internal cardiac massage is also indicated to manually pump the empty heart while volume is infused.
Diagnostics & Findings
- Rhythm check (Sinus Tachycardia without a pulse -> PEA)
Findings:
- Loss of pulse (PEA arrest)
- Systolic BP dropped to 68 before arrest
- Heart is empty of volume on direct visualization
Interventions
- Initiated CPR (Chest compressions)
- Left anterolateral resuscitative thoracotomy performed
- Placed rib spreader
- Cross-clamped the descending aorta using a Satinsky clamp
- Initiated internal open-chest cardiac compressions
- Administered units 7 and 8 of whole blood on rapid infuser
⮑ Outcome & Reassessment
Aorta successfully cross-clamped. The team actively performing internal cardiac massage while aggressively pushing more whole blood to refill the empty vascular system.
Clinical Media


ROSC & Disposition
Reassessment of cardiac filling and pulse during internal compressions.
ROSC & Disposition
Reassessment of cardiac filling and pulse during internal compressions.
Medical Decision Making
With the aorta clamped, the rapid infusion of whole blood has successfully refilled the patient's thoracic vasculature. The heart is visibly filling and beating effectively on its own again. A strong radial pulse has returned, and the systolic blood pressure is stabilizing around 94. The ED has accomplished maximal stabilization; the patient must now be transferred immediately to the Operating Room so the vascular surgeon can definitively repair the ruptured AAA and the chest can be formally closed.
Diagnostics & Findings
- Pulse check
- Direct visualization of myocardial filling and contractility
Findings:
- Return of strong radial pulse
- Systolic BP of 94
Interventions
- Placed moist lap pads over the open thoracotomy incision
- Packaged patient with rapid infuser and extra blood for immediate transport
- Transferred patient to the Operating Room (OR)
⮑ Outcome & Reassessment
Patient achieved ROSC. Hemodynamics temporarily stabilized with the aortic cross-clamp in place. Transferred to OR.
Post-Mortem Chart Review
Restoration of the Electronic Health Record (EHR) system allows for retrospective review of the patient's medical history following his death in the OR.
+1
Post-Mortem Chart Review
Restoration of the Electronic Health Record (EHR) system allows for retrospective review of the patient's medical history following his death in the OR.
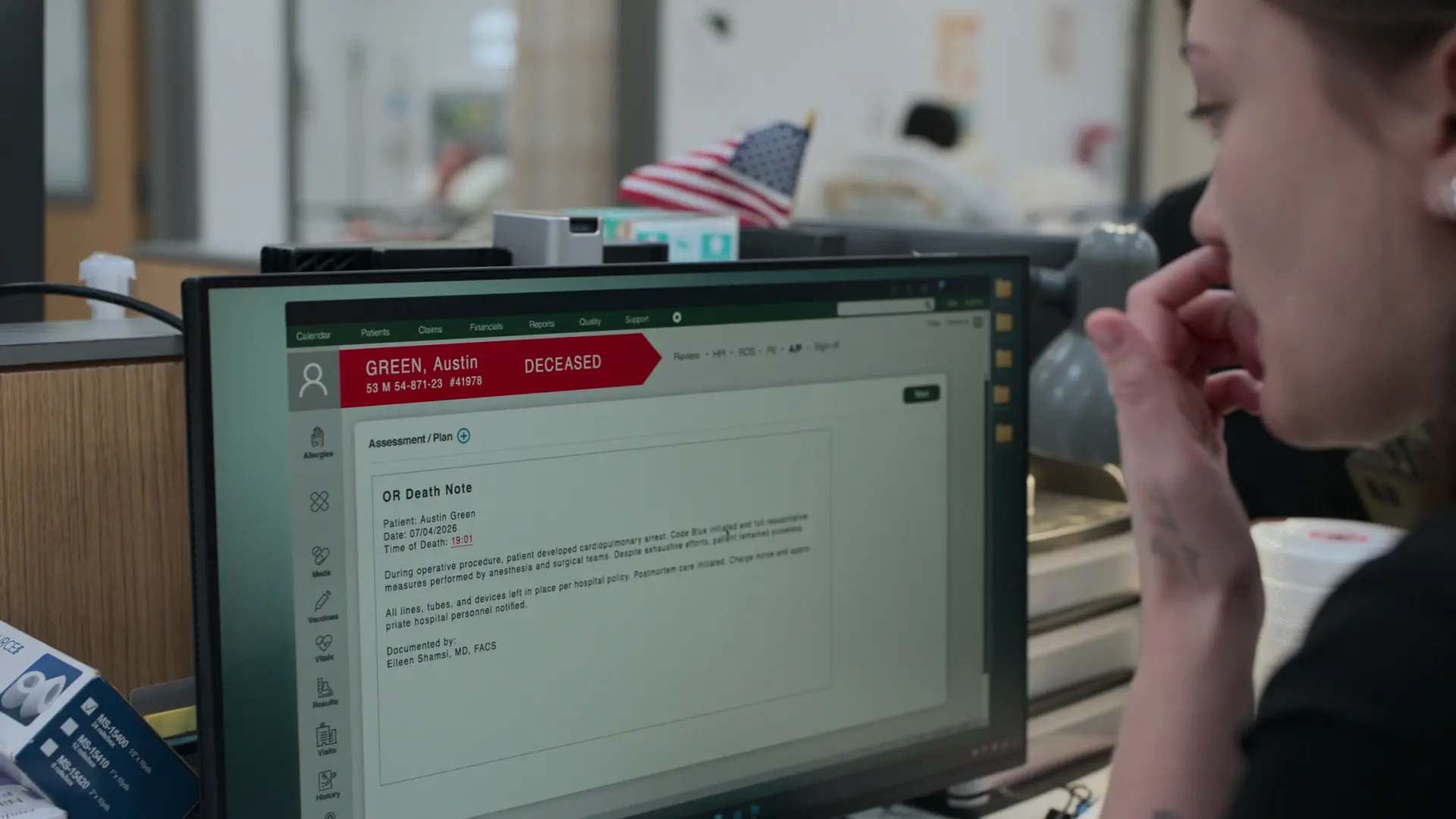
Medical Decision Making
With the hospital's computers and Electronic Health Record (EHR) systems back online, the staff can finally access the patient's full medical history. The review reveals that the patient expired on the operating table at 19:01 due to intraoperative cardiopulmonary arrest. Crucially, the chart shows a CT scan from 1.5 years ago documenting a 4-centimeter AAA. At that time, it was too small for surgical intervention, and routine 6-month surveillance ultrasounds were recommended. The patient was lost to follow-up. Because the ED team had no access to the EHR during the cyberattack and the patient failed to report it, the team was completely blind to this high-risk pre-existing condition, leading to the devastating anchoring bias on his kidney stone history.
Diagnostics & Findings
- Retrospective Electronic Health Record (EHR) chart review
Findings:
- Time of death: 19:01
- Prior CT scan (18 months prior) documented a 4cm Abdominal Aortic Aneurysm
- Patient failed to attend recommended 6-month surveillance ultrasounds
Interventions
- Postmortem care initiated per hospital policy
⮑ Outcome & Reassessment
Patient expired in the Operating Room. Code Blue initiated intraoperatively but resuscitative efforts were unsuccessful.
Clinical Media
Diagnoses & Disposition
Evolving Diagnoses
- [Season 02, Episode 09]Left Ureteral Calculus (Renal Colic) with Mild Hydronephrosis
- [Season 02, Episode 11]Ruptured Abdominal Aortic Aneurysm (AAA) (Initially misdiagnosed as uncomplicated renal colic)
- [Season 02, Episode 13]Deceased: Hemorrhagic shock secondary to ruptured 8cm Abdominal Aortic Aneurysm (AAA) - Expired in OR
Current Disposition
Deceased. Patient expired in the Operating Room during attempted definitive surgical repair of his ruptured Abdominal Aortic Aneurysm.
Casebook Analysis
Episode Context
Austin Green's arc transitions from a standard 'bread-and-butter' medical case to a devastating tragedy that underscores the vulnerability of the healthcare system. Initially serving to highlight ED throughput issues and the chaotic effects of an attending's absence in S02E09-E10, the plot catastrophically twists in S02E11 when his 'kidney stone' reveals itself as a ruptured AAA. In S02E13, the arc resolves tragically: Green dies in the OR. The revelation that his AAA was previously known but missed due to a hospital cyberattack provides a powerful commentary on medicine's reliance on Electronic Health Records (EHR) and the fatal consequences of patients failing to adhere to longitudinal surveillance.
Attending's Review
Medical Accuracy
The medical depiction of this case remains highly accurate through its tragic conclusion. The initial diagnostic pathway for renal colic was standard. The missed AAA is a classic, notorious board exam pitfall: an expanding AAA irritating the ureter mimics a kidney stone. The resuscitation with MTP, TXA, Calcium Gluconate, and the 'Hail Mary' resuscitative thoracotomy with aortic cross-clamping were incredibly realistic representations of trauma salvage maneuvers. In S02E13, the revelation that a 4cm AAA grew to 8cm over 1.5 years without surveillance is medically sound; AAAs can expand unpredictably, which is exactly why 6-month surveillance is mandated for aneurysms of that size.
Complications & Errors
- Administrative Delay: Patient's discharge is prolonged due to the pharmacy being backed up and the primary attending physician (Dr. Mohan) being temporarily unavailable to sign the final discharge orders.
- Diagnostic Error / Anchoring Bias: Student Doctor Ogilvie and Dr. Mohan anchored prematurely on the patient's history of kidney stones, the presence of hematuria, and mild hydronephrosis. They failed to visualize the abdominal aorta during the initial POCUS, missing a massive 8cm AAA.
Clinical Pearls
Bedside ultrasound (POCUS) is an incredibly valuable, radiation-free tool for identifying obstructive uropathy (hydronephrosis) in patients presenting with classic symptoms of renal colic.
NSAIDs (such as Ketorolac) are often superior to opioids for acute renal colic because they decrease ureteral smooth muscle tone by inhibiting prostaglandin synthesis, tackling the root cause of the pain.
A normal BUN and creatinine in the presence of unilateral hydronephrosis is reassuring; it indicates that the patient does not have a post-renal acute kidney injury, as the contralateral kidney is compensating adequately.
Disposition delays (such as awaiting prescriptions or an attending physician's final sign-off) are a major contributor to ED boarding and overcrowding, limiting bed availability for incoming acute patients.
A ruptured Abdominal Aortic Aneurysm (AAA) is a classic mimic of renal colic. An expanding AAA can irritate the ureter, causing microscopic hematuria and flank pain. Always evaluate the aorta during a renal POCUS in older patients with flank pain.
During a Massive Transfusion Protocol (MTP), calcium replacement is critical. The citrate anticoagulant in stored blood chelates the patient's serum calcium, leading to hypocalcemia which worsens shock and decreases cardiac contractility.
According to Poiseuille's Law, flow is proportional to the radius to the 4th power and inversely proportional to catheter length. Therefore, a short, large-bore peripheral IV (like a 14G or 16G) delivers fluids much faster than a standard long central venous catheter.
Normal AAA growth rate is typically 0.2 to 0.3 cm per year, but can be unpredictable. A 4cm aneurysm requiring 6-month surveillance can rapidly expand and rupture if the patient is lost to follow-up.
An abdominal aortic aneurysm (AAA) measuring 4.0 cm is typically not indicated for elective surgical repair, as the morbidity of surgery outweighs the risk of rupture. The standard threshold for elective repair is a diameter of ≥ 5.5 cm in men (or ≥ 5.0 cm in women), or rapid expansion (> 0.5 cm in 6 months). For a 4.0 cm AAA, standard management involves cardiovascular risk modification and routine surveillance with duplex ultrasound every 6 to 12 months to monitor for dangerous expansion.
Electronic Health Record (EHR) downtime is a high-risk period for medical errors. Without access to longitudinal patient histories, providers are forced to rely entirely on patient recall, leaving them highly vulnerable to missing critical pre-existing conditions.


