History of Present Illness
Patient was brought to the ED by a friend via private vehicle. The friend reports the patient tripped over rebar and hit his head. The patient initially refused to let the friend call 911 and was conversant, but his mental status deteriorated significantly en route to the hospital. Triage assessment noted a fruity, ketotic odor on the patient's breath.

Emergency Department Course
Triage & Initial Assessment
Patient brought in by friend, unresponsive to verbal commands.
+1
Triage & Initial Assessment
Patient brought in by friend, unresponsive to verbal commands.
Medical Decision Making
Patient has a history of head trauma but also has ketones on his breath. It is unclear if he fell because he was altered from an underlying metabolic issue (like DKA) or if he is altered due to a traumatic brain injury. Needs immediate trauma and medical resuscitation.
Diagnostics & Findings
- Olfactory assessment (smelled ketones)
Findings:
- Ketones on breath
- Altered mental status
Interventions
- Activated Code Trauma Tier One overhead
⮑ Outcome & Reassessment
Patient remains unresponsive; moved immediately to Trauma Bay.
Clinical Media
Primary Survey & Resuscitation
Arrival in Trauma Bay for Tier One Trauma activation.
Primary Survey & Resuscitation
Arrival in Trauma Bay for Tier One Trauma activation.
Medical Decision Making
Must rule out immediate life-threatening traumatic injuries while simultaneously evaluating for severe hyperglycemia/DKA. Abdomen is soft but patient is profoundly altered (did not flinch for IV), meaning serial exams or imaging will be needed to definitively rule out occult injury.
Diagnostics & Findings
- E-FAST exam
- Point-of-care Accu-Check (Capillary Glucose)
- Neurological exam (Plantar reflex)
Findings:
- Lung sliding present bilaterally
- Good bowel sounds, abdomen soft/non-rigid
- Toes down bilaterally (negative Babinski), no upper motor neuron deficits
- E-FAST negative
- Blood glucose > 500 mg/dL (Critical High)
Interventions
- Peripheral IV access established
⮑ Outcome & Reassessment
Point-of-care glucose confirms hyperglycemic crisis. Proceeding to medical stabilization before sending for Head CT.
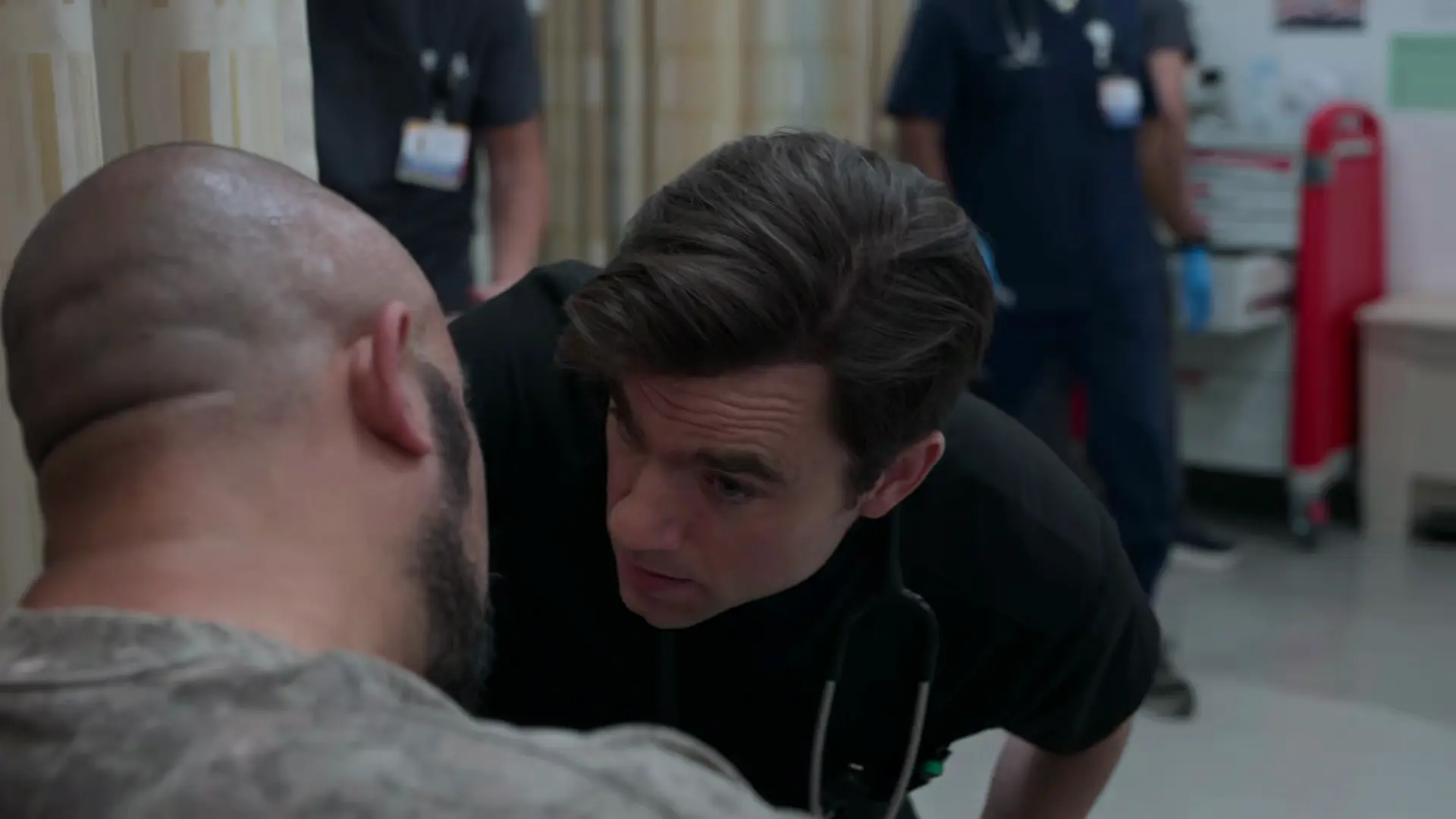
Medical Decision Making & Bedside Education
Capillary glucose over 500 mg/dL confirms hyperglycemic crisis.
Medical Decision Making & Bedside Education
Capillary glucose over 500 mg/dL confirms hyperglycemic crisis.
Medical Decision Making
Student suggests starting an insulin drip at 0.1 units/kg. Javadi corrects this: Insulin causes an intracellular shift of potassium. If the patient is already hypokalemic (K < 3.5), administering insulin could induce fatal arrhythmias. Initial focus must be aggressive fluid resuscitation while awaiting the comprehensive metabolic panel.
Diagnostics & Findings
- Ordered Chem-7
- Ordered Venous Blood Gas (VBG)
- Standard DKA precipitant workup (cultures, ECG, etc.)
Interventions
- Lactated Ringers at 1 Liter per hour
⮑ Outcome & Reassessment
Fluid resuscitation initiated safely while awaiting critical lab values.
Lab Review & Treatment Escalation
Stat laboratory results return.
+2
Lab Review & Treatment Escalation
Stat laboratory results return.
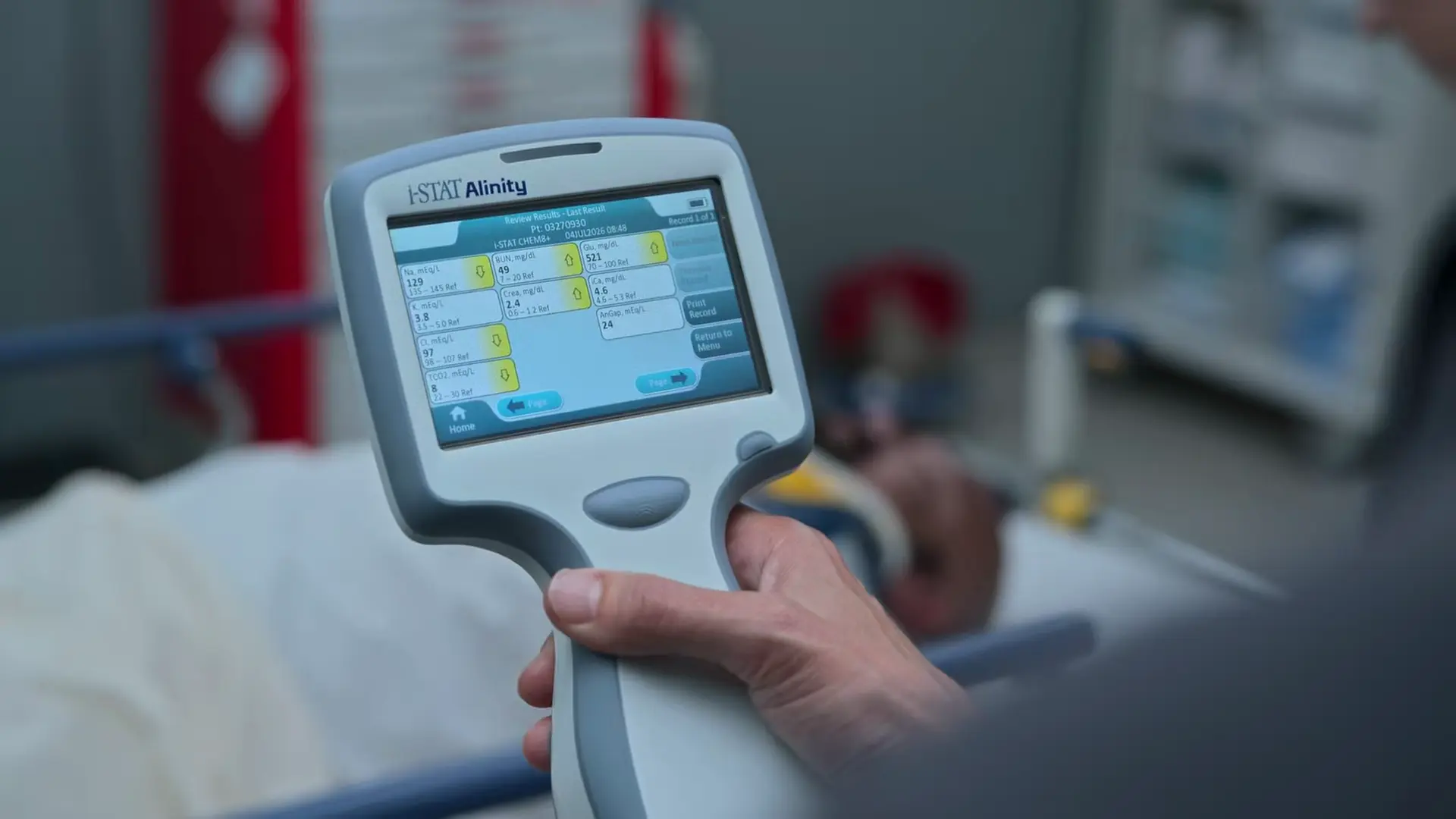
Medical Decision Making
Labs confirm severe DKA with profound acidemia (pH 6.97) and a high anion gap. Potassium is 3.7, which is safe to initiate insulin therapy, but supplemental potassium must be added to maintenance fluids to prevent insulin-induced hypokalemia as treatment progresses.
Diagnostics & Findings
- Chem-7 review
- VBG review
Findings:
- Glucose: 521 mg/dL
- Sodium: 129 mEq/L
- Potassium: 3.7 mEq/L
- Chloride: 97 mEq/L
- Bicarbonate: 8 mEq/L
- VBG pH: 6.97
- Anion Gap: 24
Interventions
- Initiate regular Insulin drip
- Add 20 mEq KCl to each liter of IV fluid
- Order capillary glucose checks every 1 hour
- Order Chem-7 every 4 hours
- Plan for double lumen midline placement for ICU transfer
- Plan for Head CT to rule out intracranial bleed
⮑ Outcome & Reassessment
Patient prepared for central/midline access and definitive ICU admission for severe DKA management.
Clinical Media
Patient Reassessment & Family Update
Patient's wife arrives at bedside; patient has regained consciousness.
+1
Patient Reassessment & Family Update
Patient's wife arrives at bedside; patient has regained consciousness.
Medical Decision Making
Patient is clinically improving but exhibits retrograde amnesia regarding his fall, which is a common finding following a concussion or a severe metabolic encephalopathy state like DKA. Medical management must continue focusing on resolving the ketoacidosis, meaning the insulin drip cannot be shut off just because he is awake.
Diagnostics & Findings
- Neurological evaluation (Mental status check)
Findings:
- Awake and alert
- Retrograde amnesia of the inciting trauma
Interventions
- Continued continuous IV insulin infusion
- Consulted hospital Case Management (Noelle Hastings) regarding uninsured status
⮑ Outcome & Reassessment
Patient is successfully resuscitated from his coma but requires ongoing hospitalization to clear serum ketones.
Clinical Media
Clinical Interview & Social Determinants of Health
Follow-up bedside visit to investigate the root cause/precipitating factor of the DKA episode.
+1
Clinical Interview & Social Determinants of Health
Follow-up bedside visit to investigate the root cause/precipitating factor of the DKA episode.
Medical Decision Making
Every episode of DKA has a precipitant (e.g., Infection, Ischemia, Infarction, Ignorance/Non-adherence). Taking a careful social history reveals the patient has been rationing his insulin (taking half doses) and infrequently monitoring his glucose due to the financial burden of test strips after losing his insurance. This identifies Financial issues as the primary etiology of his critical illness.
Diagnostics & Findings
- Social history evaluation
Findings:
- Insulin rationing (50% of prescribed dose)
- Inability to afford glucose test strips
- Loss of employer-sponsored health insurance
Interventions
- Exploration of healthcare financing options (ACA plans)
- Family discussion regarding medical expenses
⮑ Outcome & Reassessment
Patient becomes defensive and agitated when his daughter suggests a GoFundMe, highlighting the severe emotional and psychological toll that financial toxicity takes on chronic disease patients.
Clinical Media

Against Medical Advice (AMA) Attempt & Negotiation
Patient attempts to leave the hospital and remove his own IVs.
+1
Against Medical Advice (AMA) Attempt & Negotiation
Patient attempts to leave the hospital and remove his own IVs.
Medical Decision Making
Patient is in the middle of active DKA treatment; leaving now guarantees rebound crisis and potential mortality, as his blood is still highly acidotic (typically takes ~48 hours to fully clear ketones and close the anion gap). The root cause of his AMA attempt is severe financial toxicity ($100,000 in medical debt) and needing to work a second job. Instead of a hard 'no', a harm-reduction strategy is required. Negotiating a 12-hour stay allows him to exit the most critical danger zone while promising to provide outpatient resources to mitigate his panic.
Diagnostics & Findings
- Assessment of motivation
Findings:
- Patient cites $100,000 in medical debt and a second job at 4:00 PM as reasons for leaving AMA.
- Patient is still actively acidotic.
Interventions
- Counseled on pathophysiology of DKA and risks of early discharge.
- Negotiated a compromise: stay 12 more hours in exchange for home supplies and a referral to Northside Christian Health Center.
⮑ Outcome & Reassessment
Patient temporarily agrees to stay until 4:00 PM ('Okay, I guess'), buying the medical team time to continue resuscitation.
Clinical Media

Elopement & Post-Discharge Harm Reduction
Dr. Mohan returns with the promised discharge supplies and finds the room empty.
Elopement & Post-Discharge Harm Reduction
Dr. Mohan returns with the promised discharge supplies and finds the room empty.
Medical Decision Making
Patient eloped prior to completing the negotiated 12-hour stabilization window. He remains at extreme risk of relapse into DKA. Standard procedure is to document the elopement and inform security/police, but Dr. Mohan recognizes that without his insulin and supplies, he will likely end up dead or back in the trauma bay. She opts to personally intervene off the books to prevent morbidity.
Diagnostics & Findings
- Room check (patient missing)
Findings:
- Patient eloped (Left Against Medical Advice without formal sign-out)
Interventions
- Procured an off-the-books discharge kit consisting of insulin, test strips, and electrolyte powder.
- Paid out-of-pocket to send the medical supplies to the patient's home via an Uber courier.
⮑ Outcome & Reassessment
Patient eloped. Clinical outcome is unknown.
Diagnoses & Disposition
Evolving Diagnoses
- [Triage]Altered Mental Status / Head Trauma
- [Trauma 1 (Primary Survey)]Severe Hyperglycemia / Suspected DKA
- [Trauma 1 (Lab Review)]Severe Diabetic Ketoacidosis (DKA) with profound acidemia
- [ED Boarding (S02E04)]DKA secondary to Insulin Rationing (Financial Toxicity)
- [ED Boarding (S02E07)]Left Against Medical Advice (Elopement) due to severe medical debt
Current Disposition
Eloped from ED (Left Against Medical Advice) due to financial toxicity. Dr. Mohan sent discharge supplies (insulin, test strips) to his home via courier.
Casebook Analysis
Episode Context
Orlando presents as a critical dual medical/trauma case. The scenario initially serves as a vehicle for the two medical students (Javadi and Ogilvie) to competitively showcase their medical knowledge regarding DKA protocols. In Episode 4, Orlando's case shifts from an acute critical care resuscitation to an exploration of the Social Determinants of Health (SDOH), specifically highlighting the systemic issue of financial toxicity and insulin rationing in America. In Episode 7, the storyline highlights the extreme consequences of this financial toxicity: Orlando attempts to leave AMA to work a second job to pay off $100k in medical debt. He ultimately elopes, prompting Dr. Mohan to personally purchase and Uber his life-saving supplies to his house.
Attending's Review
Medical Accuracy
The medical depiction of DKA management in this episode is highly accurate and textbook. The team correctly halts starting an insulin drip without a known potassium level, highlighting a classic and fatal pitfall in DKA management. The discussion of the pathophysiology (insulin deficiency -> lipolysis -> ketogenesis -> anion gap acidosis) and the fluid-depleted state is spot-on. Furthermore, the show accurately portrays post-concussive/metabolic amnesia upon waking. Next, identifying insulin rationing due to cost as the root cause of DKA is a highly realistic and tragic reality seen daily in US Emergency Departments. The depiction of patients leaving AMA or eloping due to financial concerns and work obligations is also a heartbreakingly realistic scenario. Dr. Mohan's statement that DKA resolution takes up to 48 hours is clinically sound, as it takes time to clear the keto-acids even after glucose normalizes. However, purchasing and Ubering prescription medications to an eloped patient's house is an extreme, unrealistic liability risk for a physician, though it dramatizes the moral injury providers face.
Complications & Errors
- Dr. Mohan sending prescription medications (insulin) via an Uber to an eloped patient's house without formal discharge documentation or bedside teaching poses massive medicolegal, safety, and temperature-control risks.
Clinical Pearls
Never start an insulin drip in a DKA patient without first checking the potassium level. Insulin drives potassium into cells; if the patient is already hypokalemic (K < 3.3 mEq/L), insulin administration can trigger fatal cardiac dysrhythmias.
The initial primary intervention for DKA is aggressive IV fluid resuscitation (usually Normal Saline or Lactated Ringers) to correct the profound dehydration caused by osmotic diuresis.
The elevated anion gap in DKA is driven by the accumulation of unmeasured ketoacids, primarily beta-hydroxybutyrate and acetoacetate. Calculated as Na - (Cl + HCO3), tracking the anion gap trend is a highly reliable marker for DKA resolution. It is far superior to urine ketones, which predominantly measure acetoacetate and can paradoxically appear to worsen as beta-hydroxybutyrate is converted back into acetoacetate during patient recovery.
Always investigate the underlying precipitant of DKA. The 'I's of DKA include: Infection, Ischemia/Infarction (MI, Stroke), Intoxication, Incision (Surgery), Infant (Pregnancy), and Ignorance/Non-compliance with insulin.
Always investigate the root cause of medication non-adherence. 'Non-compliance' is often a symptom of systemic issues like financial toxicity, lack of transportation, or health literacy deficits, rather than patient apathy.
DKA resolution is defined by the closure of the anion gap and clearance of serum ketones, not just the normalization of blood glucose. Intravenous insulin must be continued until the acidosis is fully resolved, often requiring the addition of dextrose to IV fluids to prevent hypoglycemia.
When a patient insists on leaving Against Medical Advice (AMA), the physician should employ harm-reduction strategies, negotiating for partial treatments (e.g., staying for 12 hours) and setting up close outpatient follow-up.


