History of Present Illness
53-year-old male presents post single motor vehicle collision. He drove head-on into a telephone pole. Airbags deployed. He was unconscious at the scene but woke up during transport. There is no scent of alcohol; EMS suspects syncope, seizure, or falling asleep at the wheel. Initially stable upon ED arrival, he shortly develops progressive bilateral upper extremity paresthesia and impending respiratory failure.

Emergency Department Course
Triage and Initial Assessment
EMS Handover.
Triage and Initial Assessment
EMS Handover.
Medical Decision Making
High energy mechanism. Normal vitals except for sinus tachycardia. Need to rule out medical causes of the crash (syncope, seizure, arrhythmia) and assess for hidden traumatic injuries. Strict C-spine precautions are required.
Diagnostics & Findings
- Trauma Survey (Implied)
- CT Cervical Spine (Implied, revealed later)
Findings:
- No obvious external injuries noted initially.
Interventions
- C-spine immobilization
⮑ Outcome & Reassessment
Patient directed to an ED room to await formal physician evaluation.
Primary/Secondary Trauma Survey & Handover
Standard trauma protocol to rule out concomitant life threats following CT imaging.
Primary/Secondary Trauma Survey & Handover
Standard trauma protocol to rule out concomitant life threats following CT imaging.
Medical Decision Making
In high-impact blunt trauma, it is critical to systematically clear the chest and abdomen for internal hemorrhage or pneumothorax before focusing solely on orthopedic or neurologic findings. Once the torso is cleared, attention can safely center on the isolated cervical spine injury identified on imaging.
Diagnostics & Findings
- Physical Exam (Chest and Abdomen)
- CT Cervical Spine Review
Findings:
- Chest and belly cleared ('look good').
- CT confirmed C-spine uni-facet dislocation.
Interventions
- Plan to consult Neurosurgery
⮑ Outcome & Reassessment
Patient is cleared of acute torso trauma but immediately begins reporting worsening neurologic symptoms.
Clinical Deterioration
Patient complains of worsening tingling in both arms and subjective dyspnea.
Clinical Deterioration
Patient complains of worsening tingling in both arms and subjective dyspnea.
Medical Decision Making
Bilateral upper extremity paresthesia, subjective dyspnea, and hypoxia suggest a high cervical cord lesion. CT scan confirmed a C4/C5 uni-facet dislocation. The jumped facet is compressing the spinal cord and potentially kinking vascular supply (ischemia). The worsening respiratory status indicates involvement of the phrenic nerve roots (C3-C4-C5), which control the diaphragm.
Diagnostics & Findings
- Physical Exam (Motor function)
- Review of CT Cervical Spine
Findings:
- Grip strength is 3/5 bilaterally.
- CT shows uni-facet dislocation at C4/C5.
Interventions
- 10 mg Dexamethasone IV
- Paged Neurosurgery Stat
⮑ Outcome & Reassessment
Patient continues to deteriorate, complaining of an inability to take a shallow breath and onset of lower extremity tingling.
Emergency Procedure
Sats dropping to 79%; patient loses sensation in feet and is in overt respiratory failure.
+5
Emergency Procedure
Sats dropping to 79%; patient loses sensation in feet and is in overt respiratory failure.
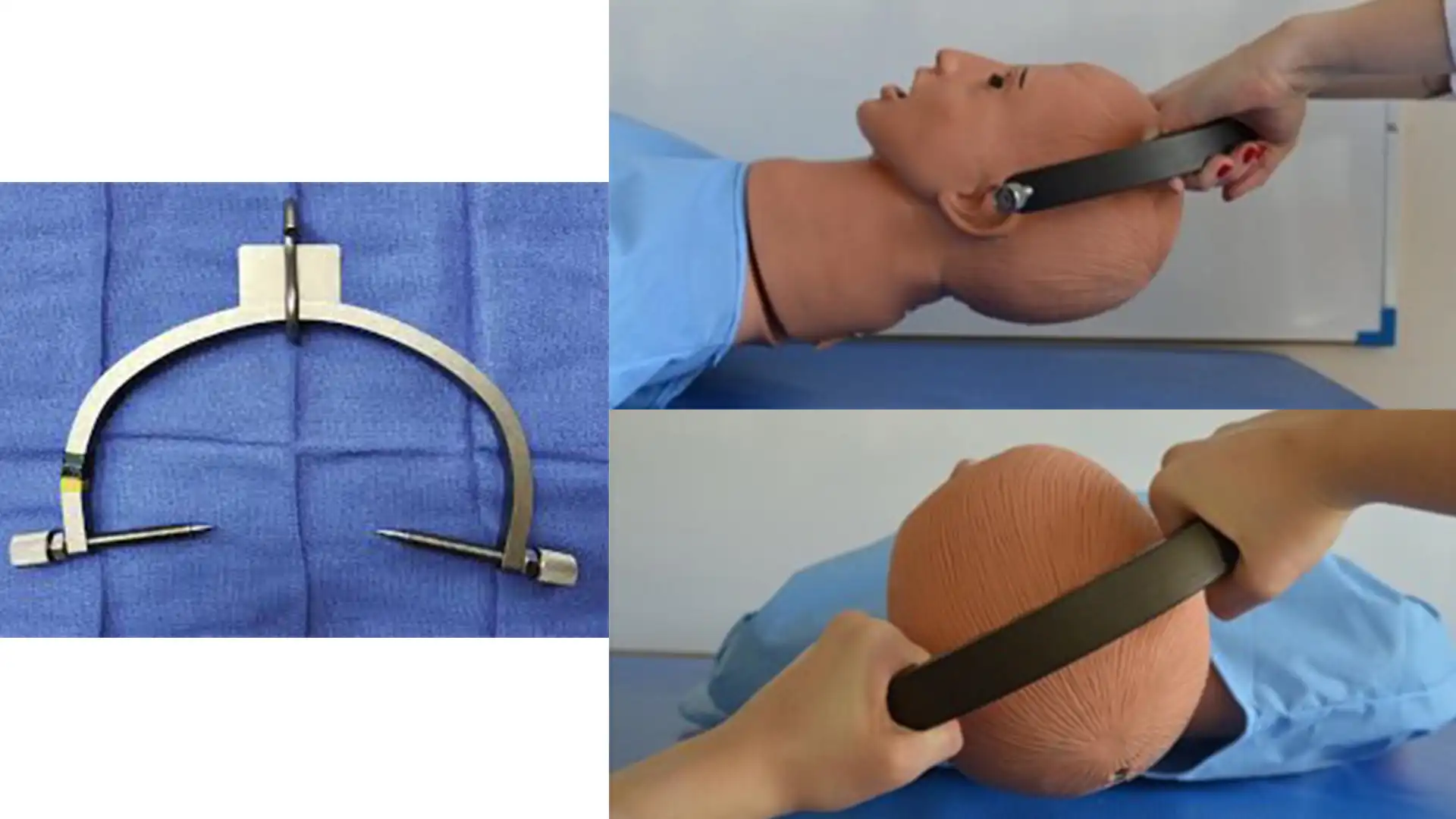
Medical Decision Making
Neurosurgery fellow is 15 minutes away. Delaying reduction will almost certainly guarantee permanent quadriplegia or death via respiratory failure. The standard of care is skeletal traction (Gardner-Wells tongs) or open surgical reduction, but we lack the time and equipment. A blind, manual closed reduction is a 'Hail Mary' with high risk of causing quadriplegia, but doing nothing carries the exact same risk.
Diagnostics & Findings
- Continuous clinical neurological monitoring during reduction
Findings:
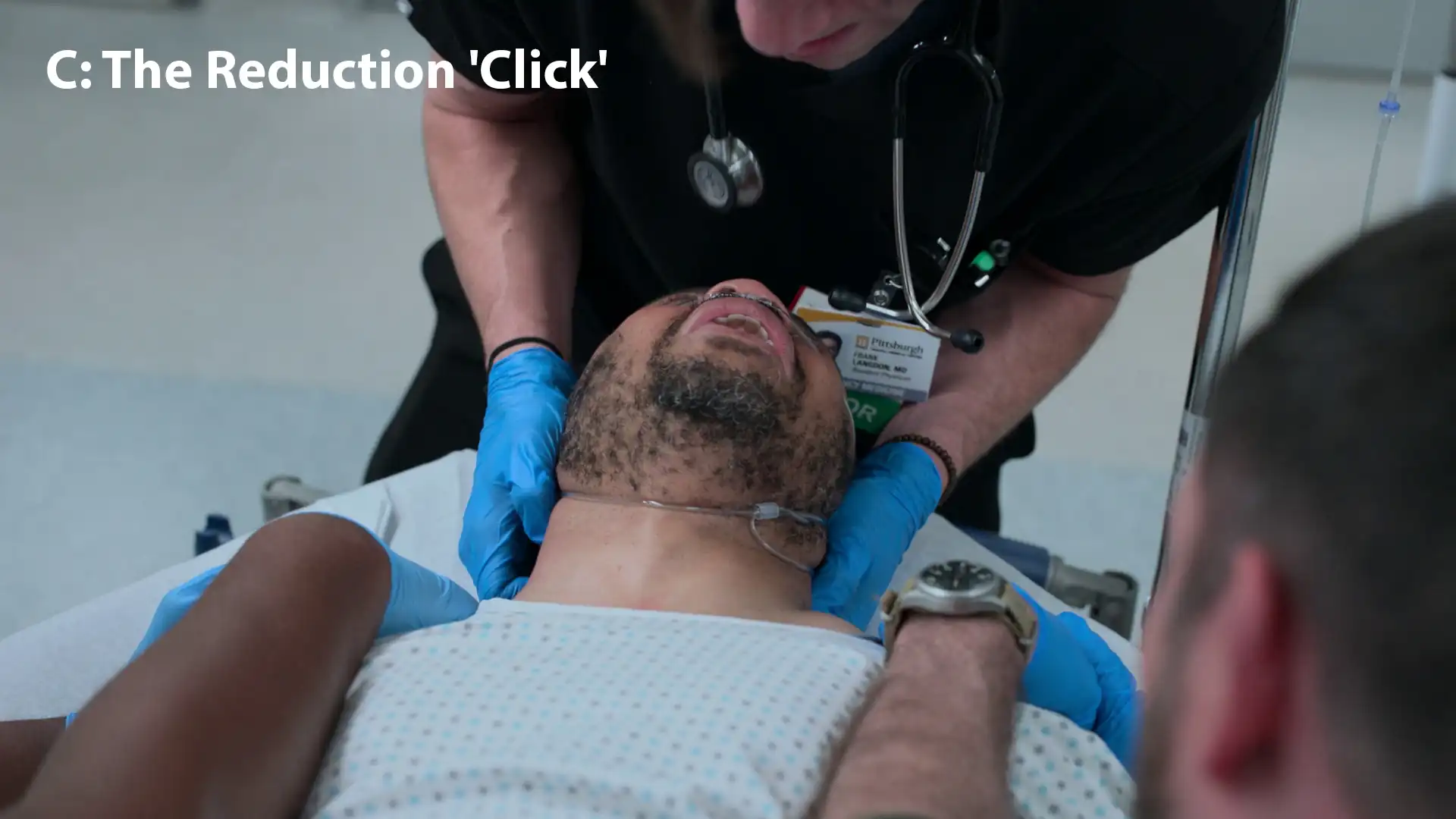
- Audible/tactile 'click' representing the un-jumping of the facet and realignment of the vertebrae.
Interventions
- 100% Non-rebreather oxygen mask
- 50 mcg Fentanyl IV
- Shoulders pinned for counter-traction
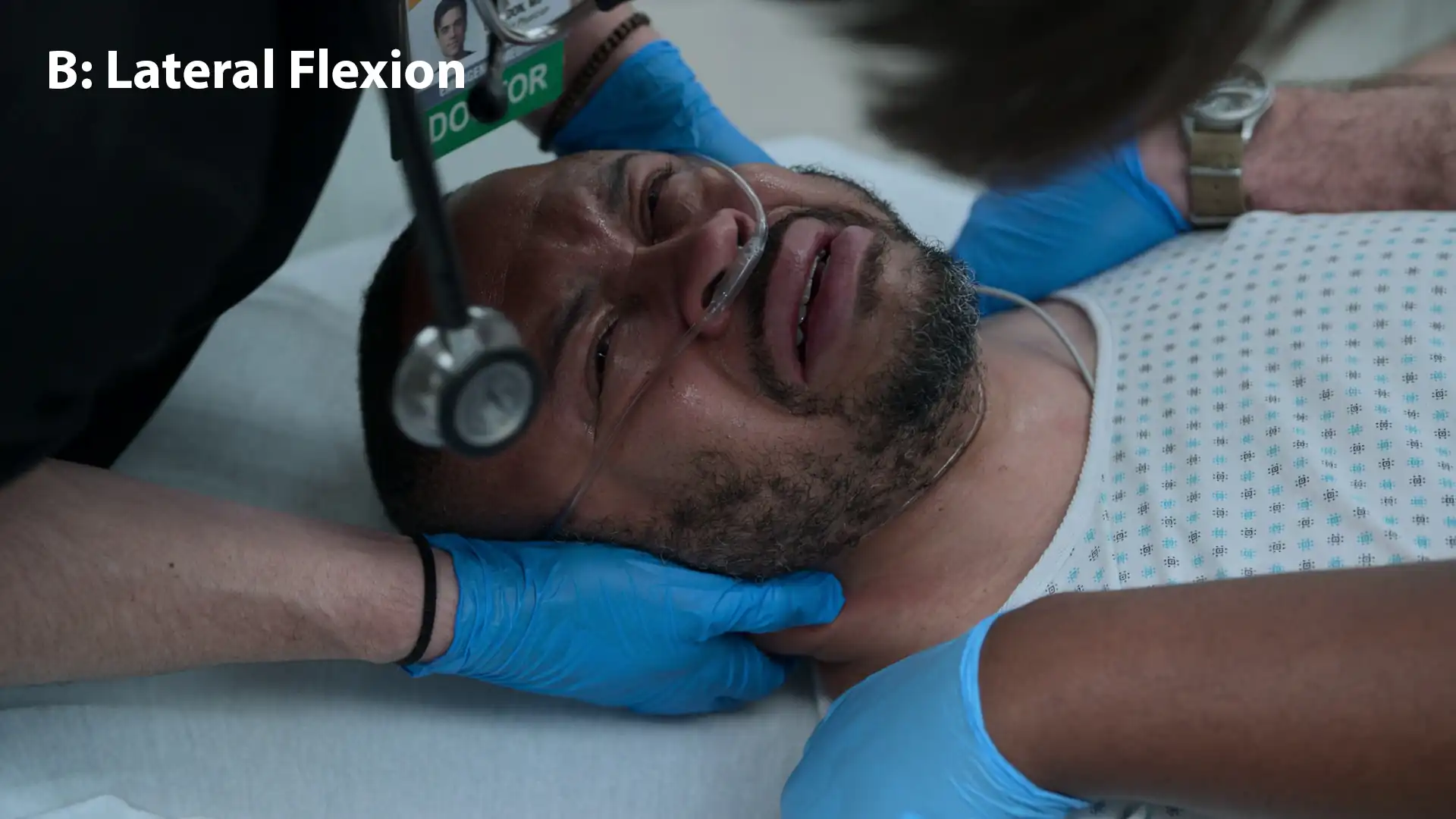
- Manual inline cervical traction, flexion to the right (to unlock the facet), followed by slight extension
- Application of a Philadelphia collar post-reduction
⮑ Outcome & Reassessment
Following the 'click', the patient immediately breathes easier. Lower extremity tingling improves. Neuro exam significantly improves. Ordered repeat CT scan prior to Neurosurgical handover.
Clinical Media


Diagnoses & Disposition
Evolving Diagnoses
- [S02E14]Uni-facet Cervical Dislocation (C4/C5)
- [S02E14]Incomplete Cervical Spinal Cord Injury with Neurogenic Respiratory Failure
Current Disposition
Stabilized in a Philadelphia collar, awaiting repeat CT scan and subsequent transfer to the OR with Neurosurgery for halo placement/definitive fixation.
Casebook Analysis
Episode Context
This case acts as a dramatic high-stakes medical climax to prove Dr. Langdon's exceptional skill right as he is dealing with a personal subplot regarding an imminent, potentially career-ending mandatory drug test.
Attending's Review
Medical Accuracy
Performing a manual closed reduction of a cervical facet dislocation in the ED with hands alone and without fluoroscopy is incredibly rare and exceedingly dangerous in modern medicine. Usually, skeletal traction (e.g., Gardner-Wells tongs) with sequential weight addition and continuous X-ray monitoring is the standard non-operative method. Doing this blindly by hand is a just 'TV doctor' moment. Additionally, the rapid reversal of severe neurologic deficits seconds after a reduction is highly dramatized; spinal cord recovery takes days to months.
Complications & Errors
- The administration of 10 mg Dexamethasone for acute blunt spinal cord trauma is an outdated practice. Since the NASCIS trials, the routine use of high-dose steroids (typically methylprednisolone, not dexamethasone) for spinal cord injury has fallen out of favor due to lack of significant proven benefit and high risks of GI bleed, infection, and hyperglycemia. Dexamethasone is usually reserved for cord compression secondary to tumors.
- Opting for a blind manual reduction instead of immediate intubation is questionable. While reducing the spine is the ultimate cure, securing the collapsing airway (RSI with inline stabilization) would typically be the immediate priority when SpO2 drops to 79%.
- The timing and sound of the reduction 'click' are dramatized. The physical unlocking and palpable 'clunk' of a jumped facet typically occurs during the active traction and lateral flexion/rotation phase, as the articular process clears the bony hurdle. The episode delays a loud, cracking sound until the final slight extension phase, treating it more like a cinematic chiropractic adjustment rather than a controlled orthopedic reduction.
- The patient's respiratory status improves immediately upon reduction, with SpO2 rising from 79% to 98% and the patient speaking in full sentences. While reduction does relieve the mechanical compression on the spinal cord, such a rapid and complete reversal of severe neurogenic respiratory failure is highly unlikely. Neurologic recovery from acute spinal cord injury is typically a slow process measured in days to months, not seconds.
Clinical Pearls
The use of corticosteroids (10mg Dexamethasone IV) in acute spinal cord injury is a historically debated topic. While Dr. Langdon orders 10 mg Dexamethasone to reduce cord edema, modern trauma protocols advise against the routine use of steroids for blunt spinal trauma due to a high rate of complications and poor evidence of long-term neurologic benefit. Furthermore, Dexamethasone targets vasogenic edema (typically seen with spinal tumors), whereas trauma causes cytotoxic edema.
'C3, C4, C5 keeps the diaphragm alive.' High cervical injuries commonly present with progressive diaphragmatic paralysis due to phrenic nerve involvement. Always anticipate the need for early mechanical ventilation.
A uni-facet dislocation occurs via a flexion-rotation mechanism and typically causes a 25% anterior translation (subluxation) of the vertebral body on imaging. A bi-facet dislocation usually causes >50% translation.
In rapidly progressive cervical myelopathy, 'Time is Spine'. Prompt decompression (either via closed skeletal traction or open surgery) is paramount to preserving neurological function.
In a true clinical setting, closed reduction of a cervical facet dislocation is rarely performed blindly by hand. Instead, Gardner-Wells tongs are pinned to the skull. Weights are then sequentially added to a pulley system under continuous fluoroscopic (X-ray) and neurological monitoring to safely achieve axial distraction and realignment.


