History of Present Illness
Orlando Diaz is a patient who was previously admitted for Diabetic Ketoacidosis (DKA). He eloped Against Medical Advice (AMA) because he could not afford to miss a paycheck at his second job. Shortly after leaving, he fell approximately 20 feet at his worksite. He was found unresponsive by coworkers after failing to answer his radio and brought back to the ED by EMS.

Emergency Department Course
Initial Trauma Assessment
Patient arrival via EMS status post 20-foot fall.
+1
Initial Trauma Assessment
Patient arrival via EMS status post 20-foot fall.
Medical Decision Making
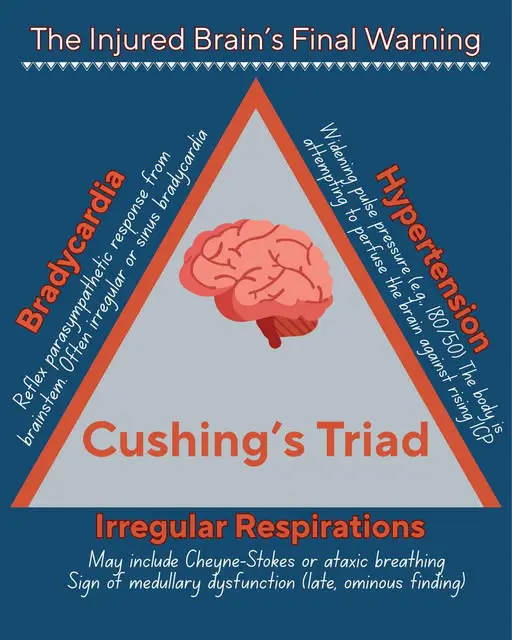
Patient presents with classic Cushing's reflex (hypertension and bradycardia), indicating dangerously increased intracranial pressure (ICP). Ruptured tympanic membrane with sero-sanguinous fluid strongly suggests a basilar skull fracture. The DKA is resolving based on the anion gap improving from 24 to 14, meaning the fall was likely due to syncope from dehydration/heat, an N-STEMI, or a posterior CVA, rather than a diabetic coma. Priority is securing the airway and stat non-contrast Head CT.
Diagnostics & Findings
- Primary Survey
- Chem-8 (Anion gap 14, Glucose 284, K+ normal)
- Stat CT Head/C-Spine/Chest/Abd/Pelvis
Findings:
- Lungs up bilaterally
- Pelvis stable
- Right tib-fib hematoma
- Deformed right forearm
- Ruptured left TM with sero-sanguinous fluid
Interventions
- C-spine immobilization
- Intubation (performed by EMS prior to arrival)
⮑ Outcome & Reassessment
Patient remains unresponsive (GCS 3) but hemodynamically stable enough for transport to the CT scanner.
Clinical Media
Post-CT Medical Management
Review of CT scan results requiring immediate neurocritical care medical management.
+1
Post-CT Medical Management
Review of CT scan results requiring immediate neurocritical care medical management.
Medical Decision Making
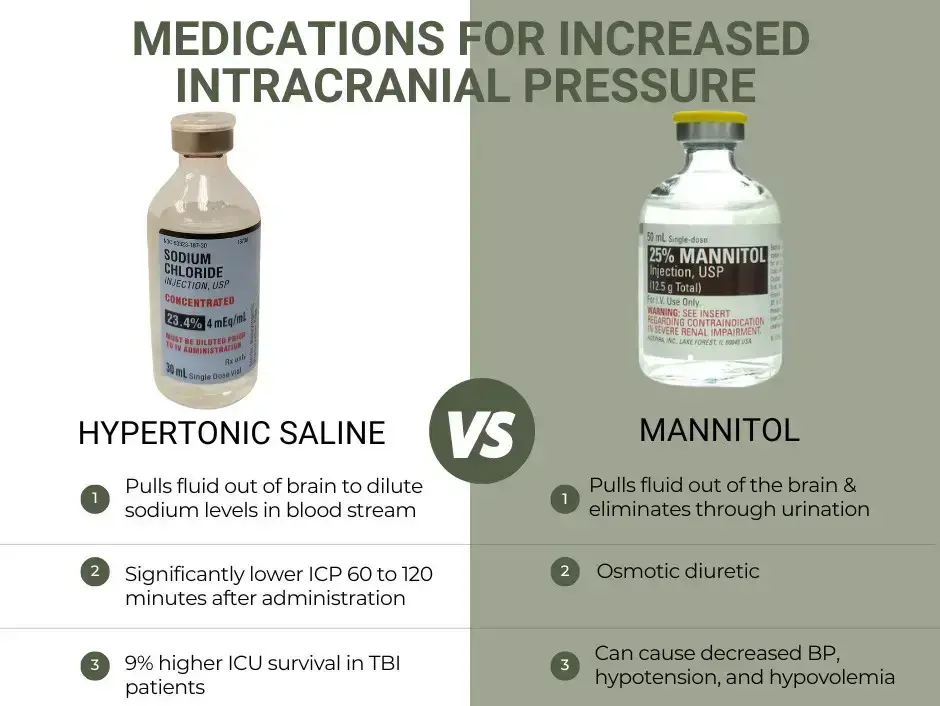
CT shows no surgical bleeds (no subdural/no epidural) but reveals diffuse brain swelling with effacement and compression of the ventricles. Medical management of elevated ICP is required. Hypertonic saline (23%) is selected over Mannitol to avoid hypovolemia/hypotension (diuresis) in a trauma patient. Anti-seizure prophylaxis is standard for severe TBI.
Diagnostics & Findings
- Review of Pan-Scan
Findings:
- No subdural or epidural hematoma
- Diffuse brain swelling with compressed ventricles
- Left pulmonary contusion
- No intra-abdominal hemorrhage
Interventions
- Placed Central Venous Pressure (CVP) line
- Placed Arterial Line
- Keppra (Levetiracetam) 20 mg/kg IV for seizure prophylaxis
- 23% Hypertonic Saline (50cc via central line) to reduce ICP
- Maintenance Lactated Ringers (LR)
⮑ Outcome & Reassessment
Despite hypertonic saline, medical management alone is not sufficient.
Clinical Media
Bedside Neurosurgical Procedure
Failure of medical management to sufficiently reduce ICP; neurosurgery consulted.
+2
Bedside Neurosurgical Procedure
Failure of medical management to sufficiently reduce ICP; neurosurgery consulted.
Medical Decision Making
To optimize Cerebral Perfusion Pressure (CPP = MAP - ICP), the ICP must be physically drained. The target ICP is <22 mmHg to predict survival, with a target CPP of 60-70 mmHg to reduce morbidity. Since the patient is too unstable, an External Ventricular Drain (EVD) will be placed at the bedside rather than waiting for the OR. Nicardipine will be titrated to maintain a Mean Arterial Pressure (MAP) of 85.
Diagnostics & Findings
- Continuous invasive blood pressure monitoring (Art line)
Findings:
- Significantly elevated ICP upon ventricular puncture
Interventions
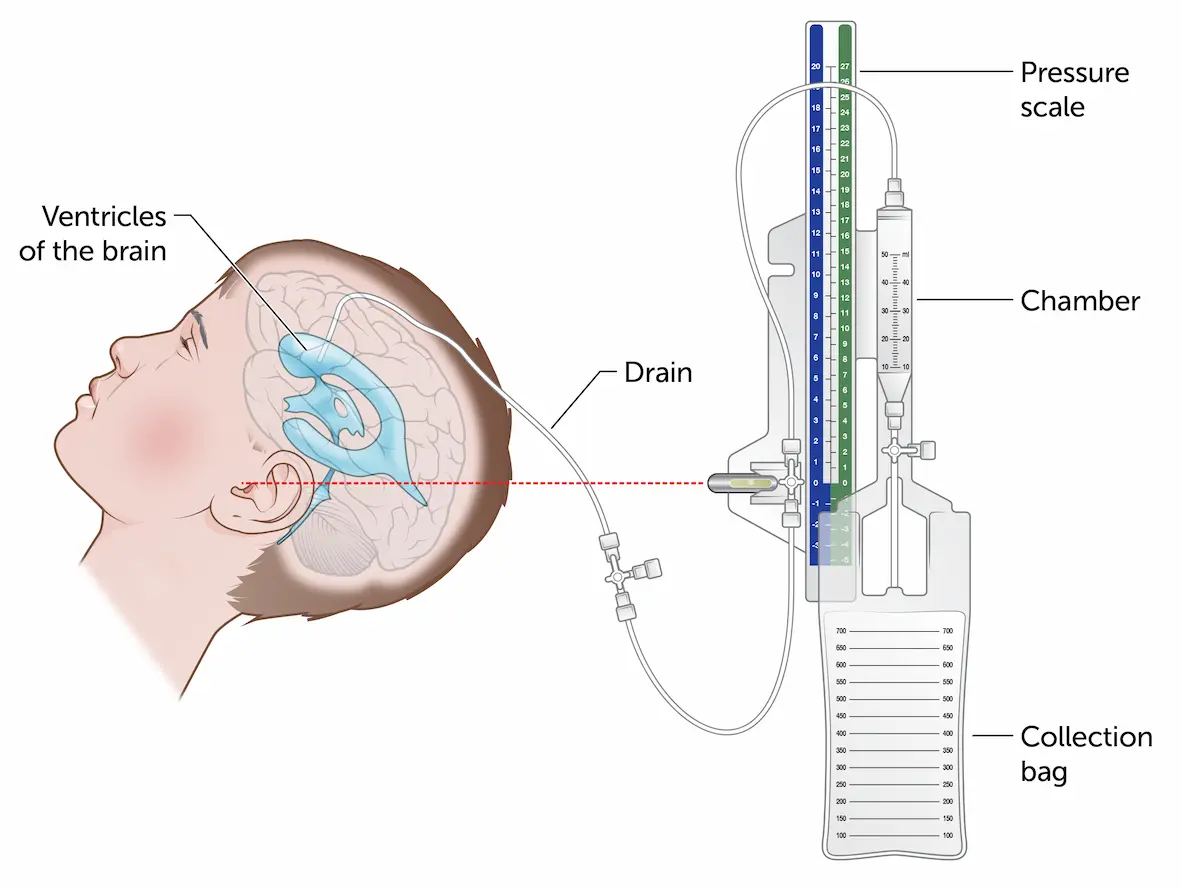
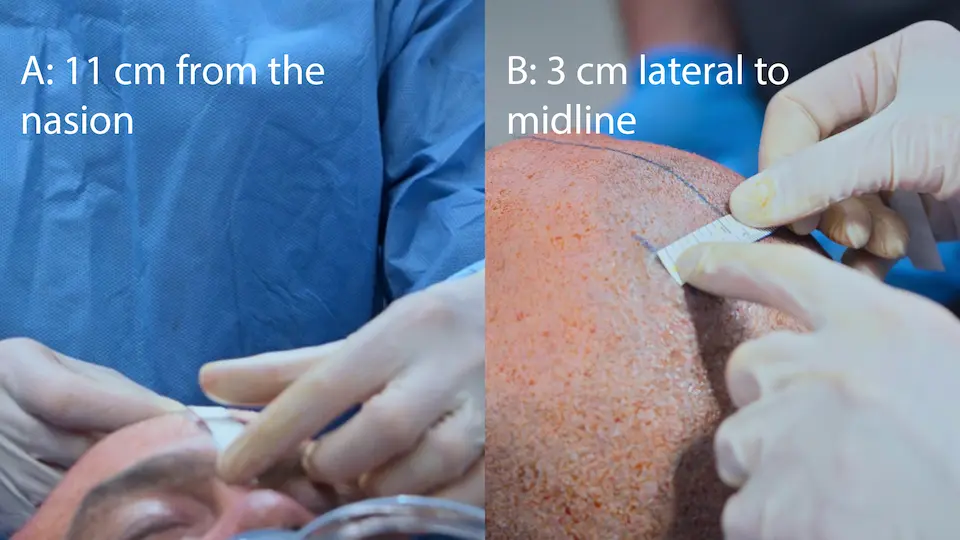
- Bedside External Ventricular Drain (EVD) placement via Kocher's point (11cm back from nasion, 3cm lateral, aimed at medial canthus)
- Nicardipine drip titrated to MAP 85
⮑ Outcome & Reassessment
EVD successfully placed. CSF drained. Blood pressure immediately improved to 190/88, HR 67. The ICP column is calibrated to zero at the level of the tragus.
Clinical Media

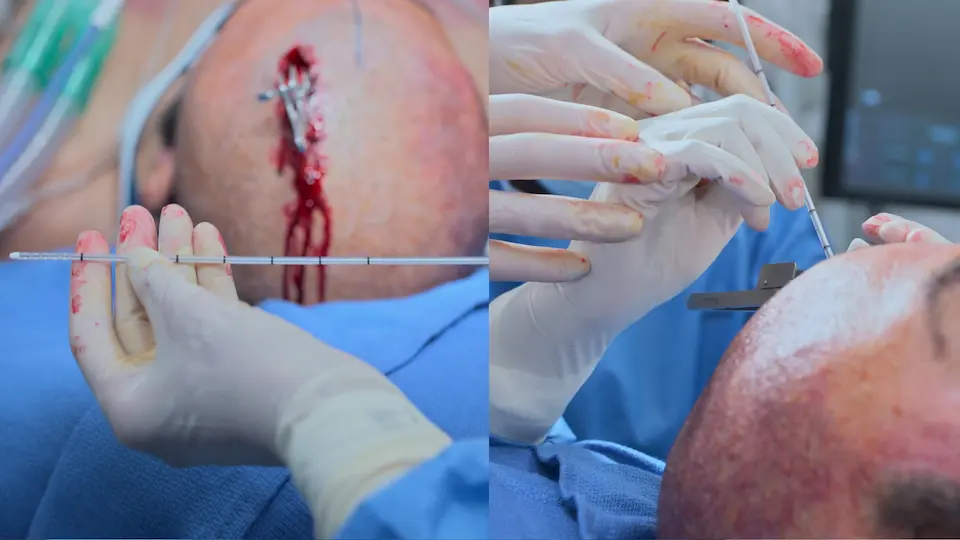
Bedside External Ventricular Drain (EVD) Placement
Execution of the bedside EVD to urgently relieve intracranial pressure.
+7
Bedside External Ventricular Drain (EVD) Placement
Execution of the bedside EVD to urgently relieve intracranial pressure.
Medical Decision Making
Using surface anatomy landmarks (Kocher's point: 11 cm posterior to the nasion, 3 cm lateral to midline) allows for a straight shot into the lateral ventricle without direct imaging guidance. The drill includes a safety stop to prevent plunging. A 'pop' feeling indicates breaching the ependymal lining, confirming ventricular access. Tunneling the catheter under the scalp for 5 cm reduces the risk of retrograde CNS infection.
Diagnostics & Findings
- Calibration of art line prior to incision
- Measurement of anatomical landmarks (Kocher's point)
Findings:
- Felt 'pop' passing the ependymal lining
- CSF successfully drained upon stylet removal
Interventions
- Incision made at Kocher's point
- Outer table of skull penetrated using hand drill (4 turns, then half turns)
- Catheter passed 5-6 cm from inner table into the lateral ventricle
- Catheter tunneled 5 cm subcutaneously to prevent infection
- Wound stapled shut
- EVD transducer calibrated to zero at the level of the tragus
⮑ Outcome & Reassessment
EVD successfully placed with immediate CSF drainage. Vitals acutely improved: BP decreased from 204/98 to 190/88, HR increased slightly to 67.
Clinical Media




Status Check & Family Discussion
Wife arrives in the ED; doctors provide prognostic update.
Status Check & Family Discussion
Wife arrives in the ED; doctors provide prognostic update.
Medical Decision Making
The patient is stabilized but comatose. For severe TBI requiring EVD and hyperosmolar therapy, prognosis is heavily guarded. Statistically, approximately 1/3 of such patients die, and 50% face long-term severe disability requiring round-the-clock care. Final prognostic outcome will not be fully clear for about two weeks.
Diagnostics & Findings
- Continuous ICP and MAP monitoring
Findings:
- MAP 85, ICP 22, CPP 63 'Best shot at survival'
Interventions
- End-of-life / Prognostic discussion with family
⮑ Outcome & Reassessment
Patient remains stable on EVD and drips. Disposition is a Neuro-Critical ICU bed once available.
Diagnoses & Disposition
Evolving Diagnoses
- [Initial Trauma Assessment]Resolving Diabetic Ketoacidosis (DKA)
- [Initial Trauma Assessment]Basilar Skull Fracture
- [Initial Trauma Assessment]Right Tib-Fib Fracture & Right Forearm Fracture
- [Post-CT Medical Management]Severe Traumatic Brain Injury (TBI) with Diffuse Cerebral Edema
Current Disposition
Admitted to the Neuro-Critical Care ICU, intubated and comatose, with an active EVD.
Casebook Analysis
Episode Context
Orlando's case is a tragic commentary on the socioeconomics of American healthcare. He originally presented with DKA but eloped because he had $100,000 in medical debt and could not afford to lose a paycheck. This directly led to his catastrophic 20-foot fall. In a dark, ironic twist, a hospital administrator later notes that if he survives with severe, long-term disability, he will finally qualify for Medicaid/Medicare, which would cover his debt and care.
Attending's Review
Medical Accuracy
The neurocritical care physiology discussed is highly accurate. The presentation of Cushing's reflex (bradycardia + hypertension) is a classic board-exam sign of impending brain herniation. The decision to use 23% Hypertonic Saline over Mannitol is completely realistic for modern trauma bays, as Mannitol's diuretic effect can cause hypotension, which is deadly in a multi-trauma patient. The landmark description for Kocher's point (11 cm posterior to the nasion, 3 cm lateral to midline) for bedside EVD placement is anatomically precise.
Complications & Errors
- During a status check at 00:33:05, Nurse Mateo reports 'CPP 22'. If the Cerebral Perfusion Pressure (CPP) is 22, the patient is actively experiencing severe global brain ischemia (target CPP is 60-70). Mateo/Production likely missed it and almost certainly meant 'ICP 22' (which aligns with the earlier stated target of keeping ICP < 22).
Clinical Pearls
Continuity of care is highly valuable in the ED, especially during shift changes or for bounce-back patients. As demonstrated when Dr. Robby and Dr. Mohan stay past their shift to treat Orlando, knowing the patient's immediate prior history (resolving DKA, recent AMA elopement, and psychosocial stressors) provides critical clinical context that aids in rapid differential diagnosis and avoids repeating redundant workups.
Cushing's Reflex (hypertension, bradycardia, and irregular respirations) is a physiological nervous system response to acutely elevated intracranial pressure and signals impending brain herniation.
The 'Halo Sign' (CSF separating from blood to form a clear ring on gauze or sheets) is traditionally taught as an indicator of a basilar skull fracture, but be cautious: it is neither highly sensitive nor specific. Saline or tap water mixed with blood can produce the exact same visual ring.
Cerebral Perfusion Pressure (CPP) is calculated as Mean Arterial Pressure (MAP) minus Intracranial Pressure (ICP). Maintaining a CPP between 60 and 70 mmHg is the cornerstone of managing severe TBI to prevent secondary ischemic injury.
CPP = MAP - ICP; To prevent secondary ischemic injury and save the brain 'penumbra', clinicians must aggressively manipulate both variables: maintaining an adequate driving pressure (MAP) while simultaneously reducing resistance (ICP) via hyperosmolar therapy or EVD drainage. The sweet spot for severe TBI is a CPP between 60 and 70 mmHg; dropping below 50 mmHg causes ischemia, while pushing above 70 mmHg risks worsening cerebral edema or inducing ARDS.
Evidence-based guidelines (such as those from the Brain Trauma Foundation) dictate strict hemodynamic thresholds in severe TBI. An ICP consistently kept below 22 mmHg strongly predicts survival and a favorable neurological outcome. Simultaneously, maintaining the CPP precisely between 60 and 70 mmHg minimizes mortality and morbidity. This narrow therapeutic window ensures the brain receives enough oxygenated blood to prevent hypoxic-ischemic injury (CPP > 60) without using excessive vasopressors that can cause systemic complications like ARDS or inadvertently worsen cerebral edema (CPP < 70).


