History of Present Illness
Patient presented overnight with symptoms suggestive of a small bowel obstruction (SBO). He has been boarding in the emergency department for over three hours waiting for a surgical consult. Initial conservative management with magnesium citrate to stimulate bowel activity failed.

Emergency Department Course
Shift Handoff
Morning sign-out from night shift.
Shift Handoff
Morning sign-out from night shift.
Medical Decision Making
Patient requires surgical evaluation to determine if conservative management is appropriate or if operative intervention is needed to clear the obstruction.
Diagnostics & Findings
Findings:
- Patient has been boarding in the ED for 3 hours pending surgery.
Interventions
- Continued observation and boarding.
⮑ Outcome & Reassessment
Patient remains in the ED waiting for definitive surgical care.
Therapeutic Intervention
Patient complains that the current treatment is not working to relieve his symptoms.
+1
Therapeutic Intervention
Patient complains that the current treatment is not working to relieve his symptoms.
Medical Decision Making
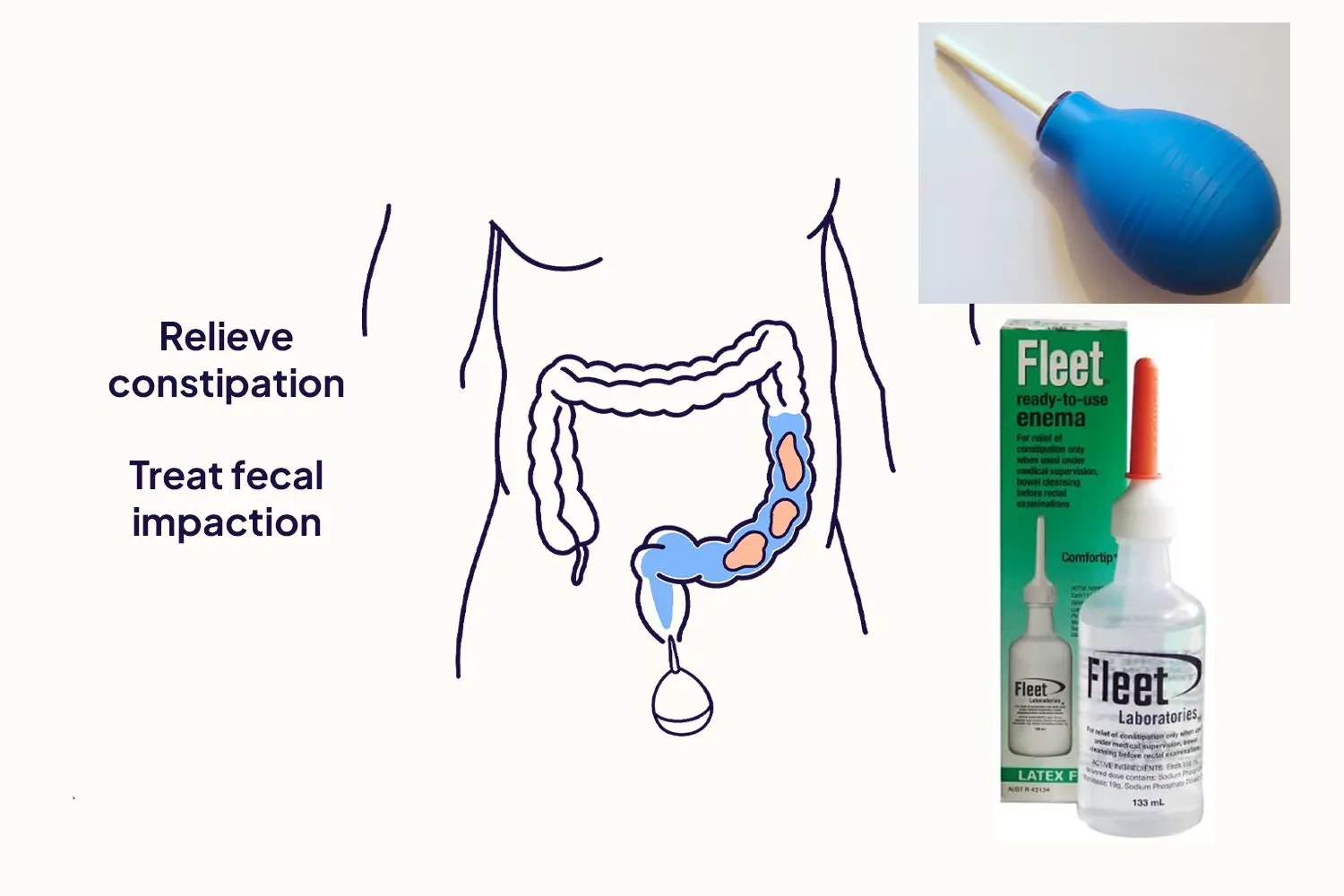
Magnesium citrate (an osmotic laxative) has failed to produce a bowel movement. A Fleet enema is ordered to provide localized osmotic pressure and lubrication to clear a potential distal impaction, assuming the obstruction is partial or lower in the GI tract.
Diagnostics & Findings
Findings:
- Lack of clinical response to oral laxatives.
Interventions
- Fleet enema ordered and administered.
⮑ Outcome & Reassessment
Patient awaits the effects of the enema.
Clinical Media
Consult Escalation
Dr. Robinavitch intercepts the surgeon to advocate for the neglected SBO patient.
Consult Escalation
Dr. Robinavitch intercepts the surgeon to advocate for the neglected SBO patient.
Medical Decision Making
The patient is at high risk for bowel ischemia and perforation due to the prolonged delay in surgical evaluation (>3 hours).
Diagnostics & Findings
Interventions
- Verbal confrontation to expedite surgical consult.
⮑ Outcome & Reassessment
The surgeon dismisses the clinical concern to tend to personal matters (visiting her daughter).
Clinical Status Update
Med student accidentally walks into the wrong patient room.
Clinical Status Update
Med student accidentally walks into the wrong patient room.
Medical Decision Making
The Fleet enema was highly effective, but the patient was unassisted and unable to reach a commode or obtain a bedpan due to severe ED understaffing.
Diagnostics & Findings
Findings:
- Patient is actively defecating into a dustpan.
Interventions
- Student quickly exits the scene.
⮑ Outcome & Reassessment
The obstruction/impaction appears to be clearing, but the patient suffers a significant discomfort due to resource shortages.
Diagnoses & Disposition
Evolving Diagnoses
- [00:04:55]Small Bowel Obstruction (SBO)
- [00:15:40]Refractory Constipation / Distal Impaction (implied by laxative/enema treatment)
Current Disposition
Still in ED (Boarding, likely resolving post-enema but still pending surgical sign-off)
Casebook Analysis
Episode Context
The patient serves a dual purpose: providing dark comic relief (the dustpan incident) while highlighting the systemic dysfunction of the hospital. The >3-hour delay for a surgical consult creates friction between ED attending Dr. Robinavitch and surgeon Dr. Shamsi, introducing inter-departmental politics.
Attending's Review
Medical Accuracy
The use of aggressive laxatives (Magnesium Citrate) and enemas (Fleet) in a true, complete mechanical Small Bowel Obstruction (SBO) is generally contraindicated due to the risk of exacerbating proximal dilation and causing perforation. However, if the clinical picture was actually a partial obstruction, an ileus, or severe fecal impaction mislabeled as an SBO, this treatment might be attempted. The 3+ hour wait for a surgical consult accurately reflects the perilous reality of ED boarding.
Complications & Errors
- Prolonged delay in surgical evaluation for an acute SBO puts the patient at risk for bowel ischemia and perforation.
- Failure of nursing staff to provide a commode or bedpan to a patient who had just received a Fleet enema, resulting in the patient defecating in a dustpan.
Clinical Pearls
True mechanical bowel obstructions require prompt surgical evaluation; do not rely solely on ED observation.
Beware of administering osmotic laxatives or enemas in patients with suspected complete mechanical bowel obstructions.
Procedure for Fleet Enema Administration: The technique varies based on who performs it. For assisted administration, place the patient in the left lateral Sims' position (left side, right knee flexed) to align gravity with the natural descending curve of the sigmoid colon; gently insert the lubricated tip pointing toward the umbilicus and squeeze slowly. For self-administration, the patient can lie on their left side or assume a knee-chest/kneeling position. In both cases, the fluid is localized to the rectum and distal colon, and the patient should retain it for 1-5 minutes until the urge to defecate is strong.
Enema Types and Mechanisms: A standard Fleet (sodium phosphate) enema is a low-volume (~133 mL) hyperosmotic solution that works by drawing water into the distal colon and rectum to stimulate peristalsis. In contrast, large-volume enemas (like tap water, normal saline, or soap suds) involve administering 500-1000+ mL of fluid via a gravity bag and rectal tube. These large-volume enemas reach higher into the descending and transverse colon to physically flush out severe or proximal impactions, but carry a higher risk of fluid/electrolyte shifts and bowel perforation.
Similar Cases from The Show


Chart Navigation
Unknown
C/OAbdominal pain, lack of bowel movements (Small Bowel Obstruction)