History of Present Illness
Patient has a lifelong history of asthma. Lost Medicaid coverage two months ago due to a missed redetermination letter, resulting in inability to afford maintenance inhalers (Symbicort, montelukast). Has only been using albuterol. Presented to the ED in severe respiratory distress after using home nebulizer every hour without relief.

Emergency Department Course
Initial Resuscitation
Sign-out presentation indicating critical status asthmaticus refractory to standard home therapy.
+1
Initial Resuscitation
Sign-out presentation indicating critical status asthmaticus refractory to standard home therapy.
Medical Decision Making
Patient is so tight that aerosolized albuterol is not penetrating the distal airways. Needs systemic bronchodilation immediately to open lungs enough for nebs to work.
Diagnostics & Findings
- Physical Exam (barely moving air, using all accessory muscles)
Findings:
- Silent chest / severely diminished breath sounds due to severe bronchoconstriction.
Interventions
- Continuous albuterol nebs at 20 mg/hr
- Epinephrine 0.3 mg IM to the thigh
⮑ Outcome & Reassessment
No immediate improvement; patient remains tight.
Clinical Media

Escalation of Therapy
5 minutes post-epinephrine, patient remains tight as a drum and is not ventilating adequately.
+1
Escalation of Therapy
5 minutes post-epinephrine, patient remains tight as a drum and is not ventilating adequately.
Medical Decision Making
Patient is approaching respiratory failure. Intubation in severe asthma carries a very high risk of cardiac arrest due to severe air trapping and decreased venous return. Must maximize all non-invasive medical avenues first.
Diagnostics & Findings
Findings:
- Persistent hypoxemia and poor ventilation.
Interventions
- BiPAP initiated (10 over 5) with in-line nebulizers
- Second dose of IM Epinephrine
- Magnesium Sulfate 50 mg/kg IV
- Aerogen vibrating mesh nebulizer ordered from the unit
⮑ Outcome & Reassessment
Continues to retract heavily. Aerogen vibrating mesh nebulizer requested to optimize 2-5 micron droplet delivery.
Clinical Media

Reassessment & Positive Response to Therapy
Evaluating patient after administration of medications via the Aerogen nebulizer system.
+1
Reassessment & Positive Response to Therapy
Evaluating patient after administration of medications via the Aerogen nebulizer system.
Medical Decision Making
The advanced vibrating mesh technology of the Aerogen created an optimal 2-to-5 micron droplet size, allowing the bronchodilator to finally penetrate the severely constricted distal airways. The patient's bronchospasm is breaking, transitioning from a 'silent chest' to expiratory wheezing, indicating improved inspiratory airflow.
Diagnostics & Findings
- Physical Exam (Auscultation)
Findings:
- Tidal volumes are noticeably up.
- Breath sounds improved; wheezes are now expiratory only.
- Patient is able to speak ('Language!') indicating significant reduction in air hunger.
Interventions
- Continued observation and medical management
⮑ Outcome & Reassessment
Significant clinical improvement. Patient is moving more air and speaking, giving the team a false sense of total resolution right before a sudden complication arises.
Clinical Media

Critical Deterioration & Misdiagnosis Averted
Patient begins tiring out and desaturating rapidly. Doctor moves to intubate.
+3
Critical Deterioration & Misdiagnosis Averted
Patient begins tiring out and desaturating rapidly. Doctor moves to intubate.
Medical Decision Making
Dr. Langdon assumes respiratory fatigue from asthma requires RSI (Ketamine/Rocuronium). Dr. Crus recognizes sudden deterioration without trauma in an asthmatic could be a spontaneous pneumothorax due to air trapping (auto-PEEP) causing alveolar rupture. Halts intubation because positive pressure ventilation would cause a fatal tension pneumothorax.
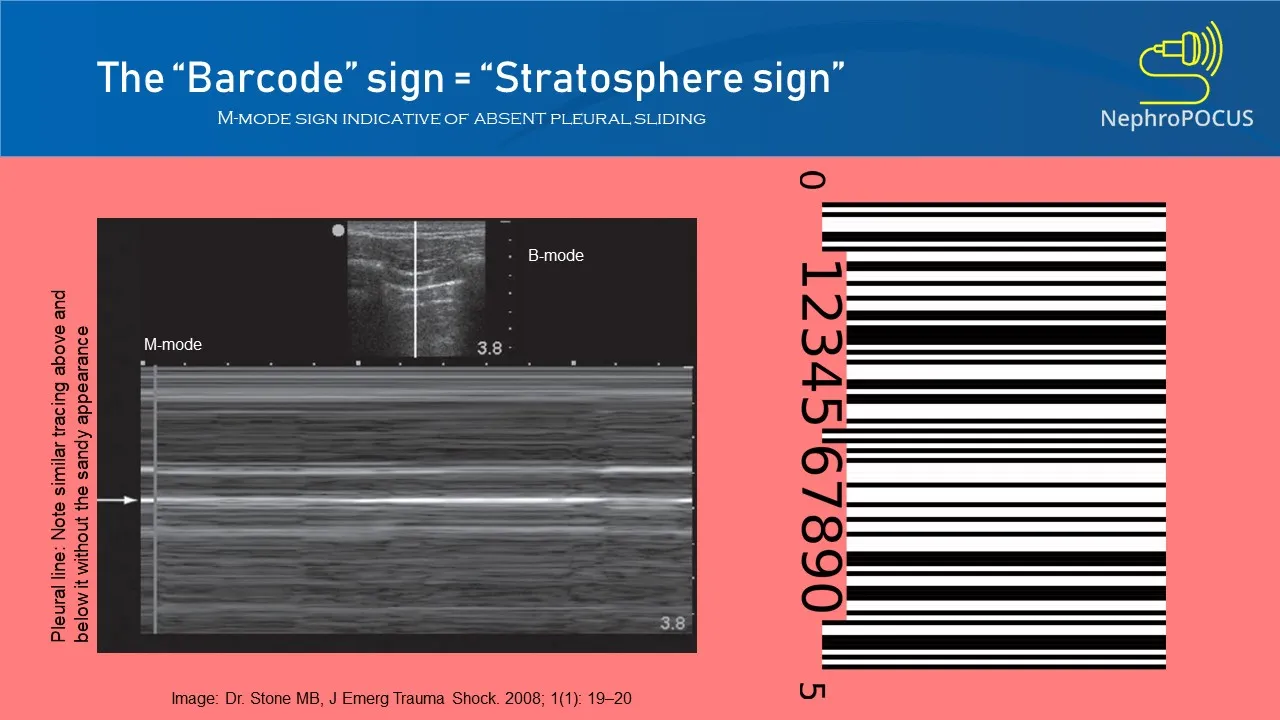
Diagnostics & Findings
- Bedside Lung Ultrasound (POCUS)
Findings:
- Absent lung sliding on the right hemithorax, confirming pneumothorax.
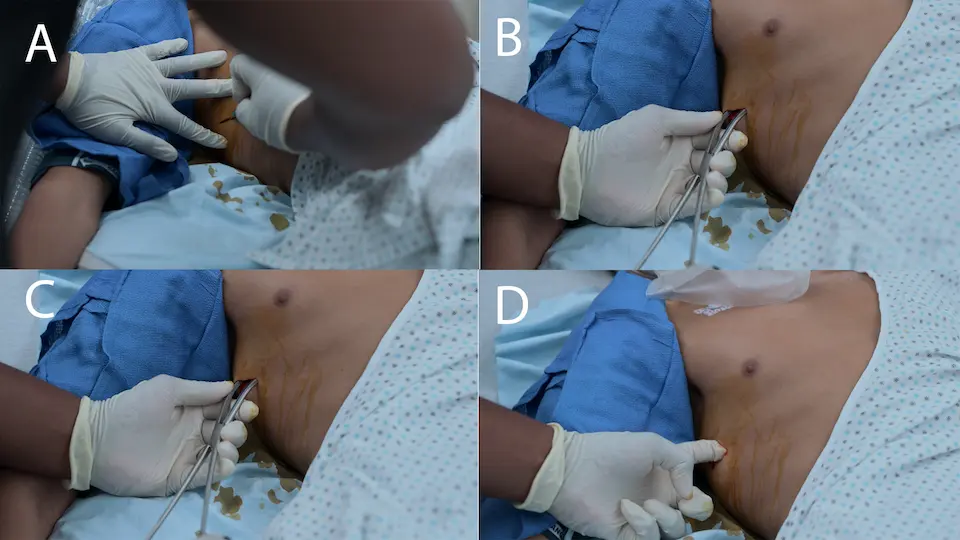
Interventions
- Intubation aborted
- Finger thoracostomy (simple thoracostomy) performed rapidly by Dr. Crus to decompress the right pneumothorax
- Implicit placement of a chest tube or pigtail catheter (off-screen) to maintain lung expansion following the initial finger sweep.
⮑ Outcome & Reassessment
Finger thoracostomy successful in rapidly releasing trapped air, averting respiratory/cardiac arrest.
Clinical Media

Reassessment & Disposition
Routine status check post-decompression and medical therapy.
Reassessment & Disposition
Routine status check post-decompression and medical therapy.
Medical Decision Making
Patient's bronchospasm has broken, and steroids are taking effect. He is oxygenating well. The underlying cause (lack of maintenance meds) must be addressed prior to discharge to prevent bounce-back.
Diagnostics & Findings
- Auscultation
Findings:
- Scattered end-expiratory wheezes (significant improvement from silent chest).
Interventions
- Systemic corticosteroids
- Social work/prescription assistance for Symbicort
⮑ Outcome & Reassessment
Patient is stable and much improved.
Diagnoses & Disposition
Evolving Diagnoses
- [Initial Resuscitation]Status Asthmaticus
- [Critical Deterioration]Spontaneous Pneumothorax (Right) secondary to air trapping
Current Disposition
Admitted for observation and continued steroid therapy. Expected discharge in 1-2 days with a new Symbicort inhaler provided by the hospital to bridge the Medicaid gap.
Casebook Analysis
Episode Context
The case highlights the systemic, real-world danger of patients losing access to preventative medications due to bureaucratic hurdles (losing Medicaid over a missed redetermination letter). Narratively, it serves to challenge Dr. Langdon, who recently returned from a 10-month absence. His near-miss with intubating a pneumothorax shakes his confidence, sparking a discussion about accepting human error and the constant pressure of Emergency Medicine.
Attending's Review
Medical Accuracy
The medical depiction is highly accurate. Intubating a patient in severe status asthmaticus is a true 'last resort' due to the extreme risk of hyperinflation, barotrauma, and hemodynamic collapse. Using IM Epi, IV Magnesium, continuous nebs, and BiPAP are all gold-standard steps to avoid the tube. Furthermore, spontaneous pneumothorax is a known complication of asthma due to alveolar hyperinflation (auto-PEEP), and catching it with POCUS before applying positive pressure is excellent emergency medicine.
Complications & Errors
- Dr. Langdon anchored on respiratory fatigue and moved straight to intubation without reassessing for pneumothorax when the patient acutely decompensated.
- If Dr. Crus had not intervened, paralyzing and applying positive pressure ventilation to the patient would have rapidly converted the simple pneumothorax into a fatal tension pneumothorax.
Clinical Pearls
Avoid intubation in asthmatics if at all possible. Maximize non-invasive options (BiPAP, Epi, Mag, Heliox) because mechanical ventilation risks severe barotrauma and hypotension.
If an asthmatic patient suddenly deteriorates or experiences a sudden drop in saturations, immediately evaluate for a spontaneous pneumothorax. Air trapping easily leads to alveolar rupture.
Bedside ultrasound (POCUS) is the fastest and most reliable way to rule in/out a pneumothorax in a crashing patient. Look for the absence of lung sliding.
Vibrating mesh nebulizers (such as Aerogen) are highly advantageous when administering bronchodilators to critically ill asthmatics on non-invasive ventilation (BiPAP). Unlike traditional jet nebulizers, they do not introduce additional gas flow into the closed circuit, preventing alterations to set pressures and FiO2, and consistently deliver an optimal 2-5 micron droplet size for maximum distal airway deposition.
For rapid decompression of a tension pneumothorax in a crashing patient, finger thoracostomy (simple thoracostomy) is increasingly the standard of care over needle decompression. Needle thoracostomy carries a high failure rate due to inadequate catheter length, kinking, or occlusion by tissue/blood, whereas a finger thoracostomy guarantees definitive pleural access, allows for tactile confirmation of the lung, and serves as the immediate precursor track for a chest tube.


