History of Present Illness
Oliver Haas is a patient with End-Stage Renal Disease (ESRD) on a Monday/Wednesday/Friday hemodialysis schedule. He missed his Friday session due to attending a wedding. His son attempted to take him to the local clinic on Saturday morning, but it was closed for the 4th of July holiday. With their local rural hospital (Pine Ridge) permanently closed, his 20-year-old son Mason drove him 1.5 hours to The Pitt. Patient arrived in extremis, exhibiting severe respiratory distress and altered mental status upon arrival.
Emergency Department Course
Triage & Initial Resuscitation
Patient arrived via private vehicle unresponsive and unable to breathe.
Triage & Initial Resuscitation
Patient arrived via private vehicle unresponsive and unable to breathe.
Medical Decision Making
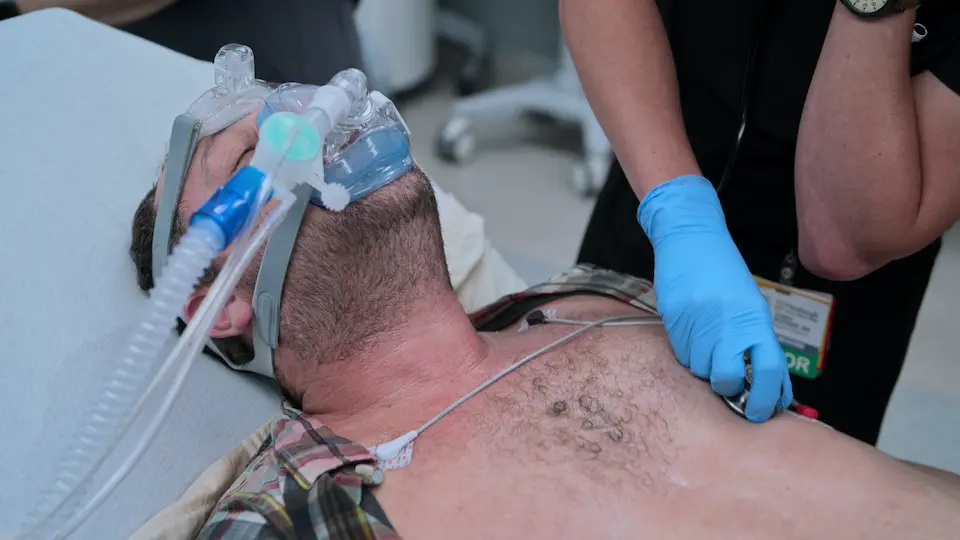
Patient is in extremis. The presence of a left-sided dialysis shunt, missed dialysis history, and profound respiratory distress strongly points to volume overload and flash pulmonary edema. Immediate airway support and afterload reduction are required.
Diagnostics & Findings
- Physical Exam (Airway check, pulse check)
Findings:
- Weak, thready radial pulse
- Altered mental status
- Left-sided dialysis shunt noted
Interventions
- Jaw thrust maneuver
- Ordered BiPAP setup
- Ordered Nitroglycerin drip ASAP
⮑ Outcome & Reassessment
Patient opens eyes to verbal stimulus. Transferred to ED bay for active management.
Diagnostic Ultrasound & Medical Intervention
Continuing severe hypoxemia despite initial maneuvers.
+2
Diagnostic Ultrasound & Medical Intervention
Continuing severe hypoxemia despite initial maneuvers.
Medical Decision Making
Patient is in Sympathetic Crashing Acute Pulmonary Edema (SCAPE). The extreme hypertension must be broken immediately to reduce afterload and allow the failing heart to pump forward. Instead of traditional low-dose, titrated nitroglycerin, we must blast with high-dose nitro (400 mcg/min) to break the sympathetic spiral rapidly.
Diagnostics & Findings
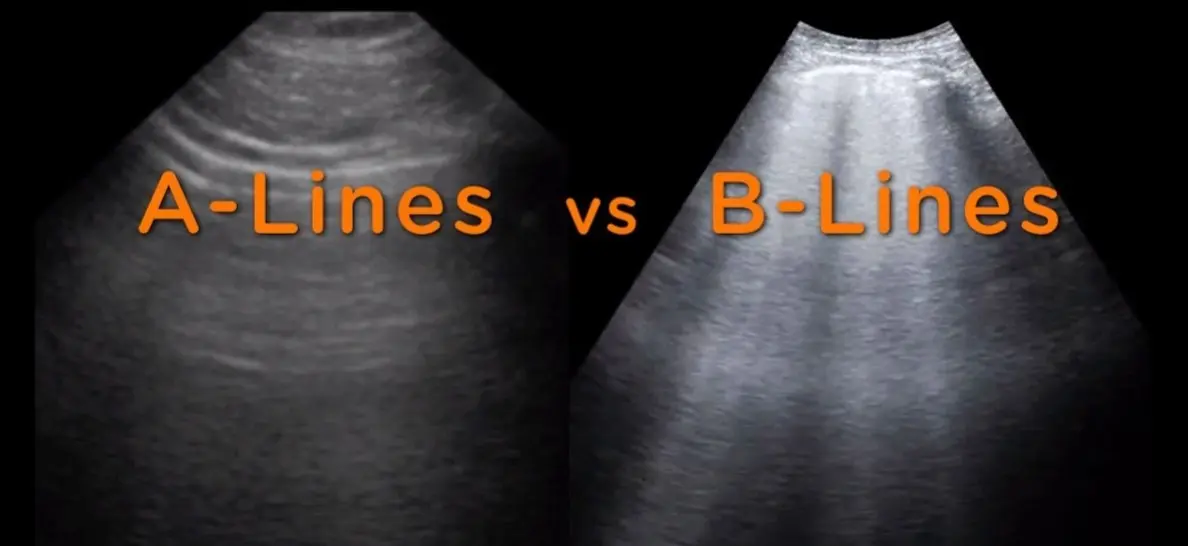
- Point-of-Care Ultrasound (POCUS) - Lung
Findings:
- Good lung sliding (rules out pneumothorax)
- Ton of B-lines bilaterally (confirms pulmonary edema)
Interventions
- Started BiPAP at 10/5
- Administered high-dose Nitroglycerin drip at 400 mcg/min for 2 to 5 minutes
⮑ Outcome & Reassessment
Pressure holds, but oxygen saturations remain dangerously low.
Clinical Media
Salvage Procedure (Therapeutic Phlebotomy)
Oxygen saturations are not improving on BiPAP; patient failing non-invasive ventilation.
+1
Salvage Procedure (Therapeutic Phlebotomy)
Oxygen saturations are not improving on BiPAP; patient failing non-invasive ventilation.
Medical Decision Making
Patient needs physical fluid removal as the kidneys are non-functional and dialysis is not immediately available. Intubation carries high morbidity in ESRD/immunosuppressed patients. Despite baseline anemia of chronic disease (Hb 9.2), a 500cc therapeutic phlebotomy is a viable, 'old school' salvage maneuver to temporarily decrease preload and the fluid burden on the lungs.
Diagnostics & Findings
- Complete Blood Count (CBC)
Findings:
- Hemoglobin: 9.2 g/dL
Interventions
- BiPAP increased to 20/10
- Therapeutic phlebotomy: 500 cc removed via 16G IV into a donor bag
⮑ Outcome & Reassessment
Fluid volume successfully removed; clinical status begins to stabilize.
Clinical Media

Lab Review & Medical Management
Basic Metabolic Panel (BMP) results return showing critical hyperkalemia.
Lab Review & Medical Management
Basic Metabolic Panel (BMP) results return showing critical hyperkalemia.
Medical Decision Making
Potassium is 6.5 mEq/L due to missed dialysis and heat stress. The ECG lacks peaked T-waves or a widened QRS, indicating the myocardium is currently stable. While Insulin/D50 is a standard treatment to shift potassium intracellularly, it carries a high risk of hypoglycemia and requires intensive nursing resources for frequent Accu-Cheks. Nebulized high-dose albuterol will shift K+ intracellularly, assist with bronchospasm/breathing, and is less resource-intensive.
Diagnostics & Findings
- Basic Metabolic Panel (BMP)
- Electrocardiogram (ECG)
Findings:
- Potassium: 6.5 mEq/L
- ECG: No peaked T-waves, no QRS widening, no ectopy
Interventions
- Deferred Insulin/Glucose
- Administered 5 mg nebulized Albuterol
⮑ Outcome & Reassessment
Treatment initiated without inducing hypoglycemia.
Reassessment & De-escalation
Scheduled clinical reassessment post-interventions.
Reassessment & De-escalation
Scheduled clinical reassessment post-interventions.
Medical Decision Making
Patient's respiratory status has significantly improved following afterload reduction, phlebotomy, and albuterol. Potassium is trending down. He can be safely stepped down from positive pressure ventilation to high-flow nasal cannula while waiting for definitive dialysis.
Diagnostics & Findings
- Repeat Basic Metabolic Panel (BMP)
Findings:
- Potassium decreased to 6.1 mEq/L
Interventions
- Discontinued BiPAP
- Initiated high-flow nasal oxygen
⮑ Outcome & Reassessment
Patient verbalizes feeling 'a little better'. Status stabilized.
Family Update & Disposition Planning
Updating the patient's son on the plan of care.
Family Update & Disposition Planning
Updating the patient's son on the plan of care.
Medical Decision Making
The acute life-threatening emergencies (SCAPE and Hyperkalemia) have been medically managed, but the underlying issue (fluid/toxin accumulation) requires hemodialysis. Patient must be admitted/observed until dialysis can be arranged.
Diagnostics & Findings
Interventions
- Admit/Observe for emergent hemodialysis
⮑ Outcome & Reassessment
Family agrees to wait in the ED. Patient remains stable.
Diagnoses & Disposition
Evolving Diagnoses
- [Triage & Initial Resuscitation]Sympathetic Crashing Acute Pulmonary Edema (SCAPE) / Acute Hypoxic Respiratory Failure
- [Diagnostic Ultrasound & Medical Intervention]End-Stage Renal Disease (ESRD) with severe fluid overload
- [Lab Review & Medical Management]Hyperkalemia
Current Disposition
Stabilized in the ED on high-flow nasal oxygen, awaiting urgent inpatient hemodialysis.
Casebook Analysis
Episode Context
Oliver's case serves as a dramatic representation of the real-world consequences of rural hospital closures. Because Pine Ridge Hospital closed due to Medicare spending cuts, his son was forced to drive him an hour and a half during a life-threatening emergency. The case highlights ED overcrowding and the ingenuity required by emergency physicians to keep patients alive when systemic resources fail.
Attending's Review
Medical Accuracy
The medical management in this case is exceptionally accurate and progressive. Using high-dose nitroglycerin (400 mcg/min) for Sympathetic Crashing Acute Pulmonary Edema (SCAPE) is a modern, evidence-based approach favored by critical care emergency physicians, countering the outdated 'start low and go slow' method. Additionally, the decision to utilize therapeutic phlebotomy as a bridge to dialysis is an old-school, physiologically sound 'salvage' maneuver that is rarely seen on TV but accurate for a desperate situation. Finally, deferring insulin/dextrose for albuterol to treat hyperkalemia without ECG changes to avoid the nursing burden of frequent Accu-Cheks reflects true-to-life ED resource management.
Complications & Errors
- No direct medical errors committed by the care team.
- Systemic complication: Delayed presentation due to the closure of the patient's local rural hospital, leading to a near-fatal cardiopulmonary crisis.
Clinical Pearls
In SCAPE, high-dose nitroglycerin is the primary intervention to rapidly reverse the afterload-driven fluid shift, whereas loop diuretics play a secondary, delayed role. Because SCAPE is typically a fluid distribution problem rather than absolute volume overload, premature diuresis can lead to hypovolemia and AKI once the sympathetic surge breaks. Furthermore, in ESRD patients like Oliver, diuretics are entirely ineffective, making rapid vasodilation and mechanical fluid removal (phlebotomy or dialysis) the only viable options.
In Sympathetic Crashing Acute Pulmonary Edema (SCAPE), do not titrate nitroglycerin slowly. Blast with high doses (e.g., 400-1000 mcg/min) to rapidly decrease afterload, allowing the failing left ventricle to pump forward.
Therapeutic phlebotomy (removing 250-500cc of blood) can act as a rapid, life-saving bridge to dialysis in patients with severe volume overload failing non-invasive ventilation, though care must be taken if the patient is severely anemic.
In hyperkalemia without malignant ECG changes, high-dose nebulized albuterol can effectively shift potassium intracellularly. This can be preferable to insulin/dextrose in a crowded ED, as it avoids the high risk of hypoglycemia and the associated nursing burden of serial blood glucose checks.


