History of Present Illness
84-year-old male who presents to the ED accompanying his wife, whom he accidentally backed his car into at low speed. The patient initially denies any injuries or complaints. However, the attending physician observes an unsteady gait, slow movements, and balance issues. The patient's daughter reports a recent decline in both parents' mobility and mentions the patient has a complex medical team ('a whole team of -ologists').
Emergency Department Course
Bedside Evaluation
Physician observation of the patient's poor mobility and stiff movements while setting up his wife's room.
+1
Bedside Evaluation
Physician observation of the patient's poor mobility and stiff movements while setting up his wife's room.
Medical Decision Making
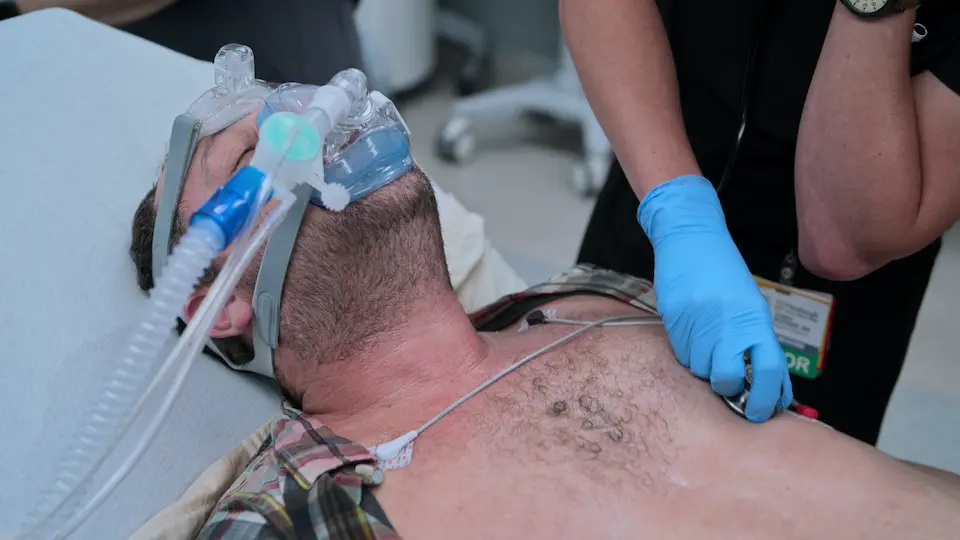
Though not the primary patient, Eddie's involvement as the driver who hit his wife raises suspicion for medical impairment. The physician initiates an 'unofficial' exam starting with basic pulmonary function and moving to a peripheral/neurological exam via the 'shoe trick' to assess for neuropathy, edema, or foot deformities common in the elderly.
Diagnostics & Findings
- Auscultation of lungs
- Visual inspection of feet and lower extremities
Findings:
- Patient struggles significantly to bend down and remove his own shoes.
Interventions
⮑ Outcome & Reassessment
Patient completes the lung exam normally but demonstrates obvious functional impairment during the physical task of removing shoes.
Clinical Media
Neurological Assessment
Continuing the opportunistic neurological workup of the impaired driver.
+1
Neurological Assessment
Continuing the opportunistic neurological workup of the impaired driver.
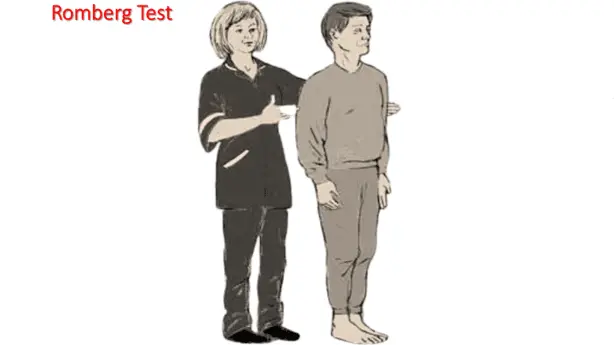
Medical Decision Making
To isolate the cause of the unsteady gait, a Romberg test is utilized. This tests proprioception and vestibular function by removing visual compensation for balance.
Diagnostics & Findings
- Romberg Test
Findings:
- Demonstrates unsteadiness.
Interventions
⮑ Outcome & Reassessment
Patient is asked to stand and maintain balance, showing signs of underlying instability.
Clinical Media
Information Gathering
Need to determine the root cause of the patient's impairment after observing family dynamics and his refusal to consider assisted living.
Information Gathering
Need to determine the root cause of the patient's impairment after observing family dynamics and his refusal to consider assisted living.
Medical Decision Making
With multiple specialists managing different organ systems, polypharmacy is a highly likely culprit for acute or subacute functional decline in a geriatric patient. The physician requests the patient's medication list from his daughter.
Diagnostics & Findings
- Medication reconciliation via family member's list
Findings:
- List obtained for review.
Interventions
⮑ Outcome & Reassessment
Daughter successfully provides the comprehensive medication list.
Medical Decision Making / Chart Review
Analyzing the obtained medication list against the patient's clinical presentation.
+2
Medical Decision Making / Chart Review
Analyzing the obtained medication list against the patient's clinical presentation.
Medical Decision Making
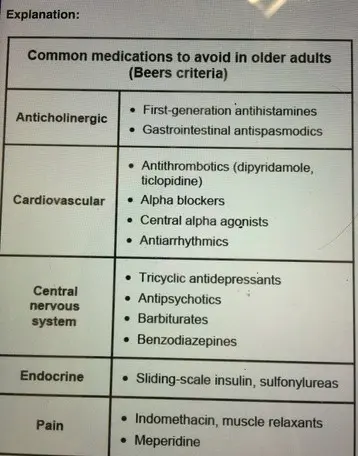
The team cross-references the patient's medications with the Beers Criteria (medications potentially inappropriate for older adults). They identify meclizine and methocarbamol, which have cumulative anticholinergic effects causing drowsiness and confusion. They also identify metoclopramide, a dopamine antagonist that frequently causes extrapyramidal symptoms (EPS) and gait abnormalities in the elderly.
Diagnostics & Findings
- Pharmacological review
Findings:
- Meclizine (Anticholinergic, causes drowsiness)
- Methocarbamol (Muscle relaxant/Anticholinergic, impairs driving)
- Metoclopramide (Prokinetic, causes EPS/gait problems)
Interventions
- Formulate deprescribing plan
⮑ Outcome & Reassessment
The clinical puzzle is solved: the patient's decline is likely entirely iatrogenic.
Clinical Media
Patient Disposition & Bedside Education
Discharging the patient and his wife with a safe, acceptable care plan.
Patient Disposition & Bedside Education
Discharging the patient and his wife with a safe, acceptable care plan.
Medical Decision Making
To preserve the patient's autonomy and dignity while ensuring safety, the physician reframes the treatment. Instead of forcing them into assisted living, she explains that his current medications are actively harming his mobility. By stopping non-critical medications and utilizing Medicare-covered home health resources, the couple can safely remain independent.
Diagnostics & Findings
Interventions
- Deprescribing of offending agents (Meclizine, Methocarbamol, Metoclopramide)
- Referral to primary care for follow-up
- Activation of case management for home PT, at-home nursing, and personal shoppers via Medicare/Area Agency on Aging.
⮑ Outcome & Reassessment
Patient is relieved that he is not being forced out of his home and expresses gratitude ('Thank you for listening'), agreeing to the home-care plan and a precautionary visit to an assisted living facility.
Diagnoses & Disposition
Evolving Diagnoses
- [Event 1]Unsteady gait of unknown etiology
- [Event 4]Iatrogenic functional decline secondary to polypharmacy (Beers Criteria medications)
Current Disposition
Discharged home. Offending medications discontinued. Enrolled in home health care and physical therapy.
Casebook Analysis
Episode Context
Eddie and his wife Frida serve as the episode's narrative device to explore the loss of independence in the elderly. Eddie's polypharmacy explains the inciting incident (him backing the car into his wife) and provides a highly satisfying diagnostic victory for Dr. Mohan, emphasizing the importance of treating the 'whole patient' rather than just the acute injury.
Attending's Review
Medical Accuracy
Highly accurate and an excellent representation of geriatric emergency medicine. Elderly patients often suffer from fragmented care where different specialists prescribe medications that interact poorly or have cumulative side effects. The specific drugs mentioned—meclizine, methocarbamol, and metoclopramide—are textbook examples of medications on the AGS Beers Criteria. Metoclopramide is particularly notorious for causing drug-induced Parkinsonism and gait instability in older adults. The solution of deprescribing rather than adding more medications is the gold standard of geriatric care.
Complications & Errors
- Fragmented Outpatient Care: The patient's primary complication arose from having 'a whole team of -ologists' who were likely prescribing medications in a silo, leading to a dangerous anticholinergic burden and dopamine antagonism without anyone noticing the cumulative effect.
Clinical Pearls
Any elderly patient presenting with a fall, functional decline, or a motor vehicle accident must have a rigorous medication reconciliation performed in the ED.
The Beers Criteria is essential for identifying potentially inappropriate medications in older adults. Cumulative anticholinergic burden (e.g., meclizine + muscle relaxants) drastically increases the risk of falls, delirium, and motor vehicle accidents.
Metoclopramide (Reglan) crosses the blood-brain barrier and acts as a dopamine receptor antagonist, which can cause severe extrapyramidal symptoms (EPS) and drug-induced Parkinsonism, often masquerading as age-related functional decline.
The 'Shoe Trick': Asking an elderly patient to remove their own shoes is a rapid, high-yield functional assessment that tests core strength, flexibility, and balance, while simultaneously granting access to perform a diabetic/neuropathic foot exam.
Polypharmacy Compounding: The intersection of meclizine, methocarbamol, and metoclopramide is a frequent Beers Criteria violations. Stacking two potent anticholinergic/CNS-depressant agents (meclizine and methocarbamol) creates a severe cumulative 'anticholinergic burden', leading to sedation, ataxia, and delayed reaction times. Combining this with metoclopramide—a central D2 receptor antagonist that crosses the blood-brain barrier and induces extrapyramidal symptoms (EPS)—creates an iatrogenic toxidrome of bradykinesia and unsteadiness that perfectly mimics severe age-related neurodegenerative decline.