History of Present Illness
Patient is a 34-year-old male who was packing class B fireworks launch tubes into a van when an explosion occurred. He was launched 10-15 feet across a garage, striking a rolled-down garage door frame. He presents with a large bleeding scalp laceration, chest pain, and tinnitus.

Emergency Department Course
Initial Assessment & Stabilization
Trauma arrival following blast injury.
+2
Initial Assessment & Stabilization
Trauma arrival following blast injury.
Medical Decision Making
Blast injuries can cause primary (overpressure wave), secondary (shrapnel), tertiary (thrown into objects), and quaternary (burns) injuries. The team must rapidly rule out internal bleeding and air-filled organ rupture. Brisk bleeding from the scalp requires rapid hemostasis to safely transport the patient to CT.
Diagnostics & Findings
- Primary Survey
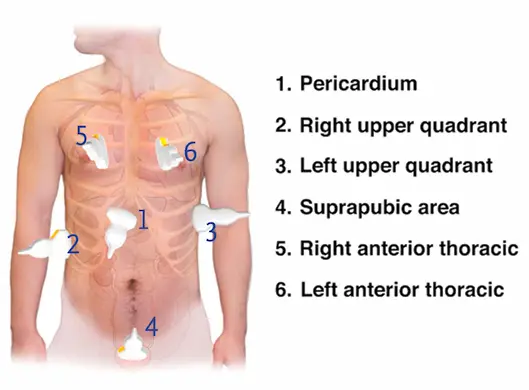
- E-FAST Exam (Negative for pericardial effusion or free fluid in belly)
Findings:
- Airway and breathing intact
- Good lung sliding bilaterally
- Tenderness over sternum (suspected fracture)
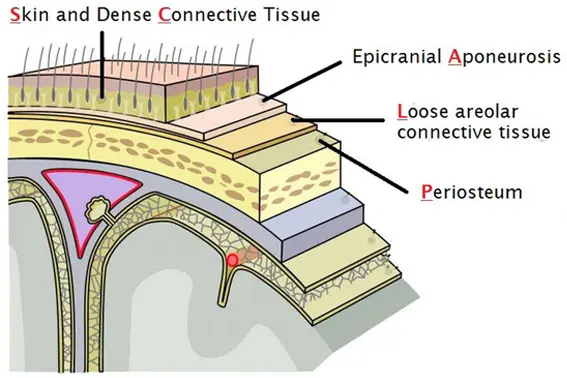
- Deep scalp laceration through the galea
Interventions
- Administered 50mcg Fentanyl
- Raney clips applied to scalp for rapid hemostasis
- Sent to CT scan
⮑ Outcome & Reassessment
Bleeding temporarily controlled; hemodynamically stable for CT transport.
Clinical Media

Post-CT Review & Procedure
Patient returns from CT for definitive wound closure.
+2
Post-CT Review & Procedure
Patient returns from CT for definitive wound closure.
Medical Decision Making
CT confirmed an isolated sternal fracture without intracranial hemorrhage. The deep scalp laceration can now be closed definitively. Given the mechanism of blunt cardiac trauma, the patient requires overnight observation for delayed dysrhythmias or complications.
Diagnostics & Findings
- CT Abdomen/Pelvis/Head/Chest
Findings:
- Isolated sternal fracture
- No skull fracture
- No intracranial hemorrhage
Interventions
- Administered 4mg Morphine
- Local anesthesia (1% Lidocaine with Epinephrine)
- Three-layer scalp closure (galea, sub-Q, skin staples)
⮑ Outcome & Reassessment
Patient is conversational, complains of chest pain with movement, but remains hemodynamically stable.
Clinical Media

Clinical Deterioration & Resuscitation
Patient complains of severe chest pain and rapidly becomes hypotensive.
+4
Clinical Deterioration & Resuscitation
Patient complains of severe chest pain and rapidly becomes hypotensive.
Medical Decision Making
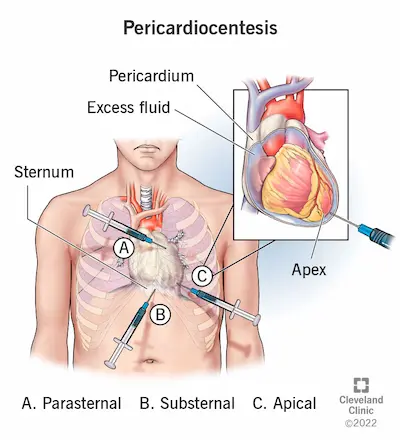
Sudden profound hypotension with JVD and clear lungs strongly suggests obstructive shock (Cardiac Tamponade or Tension Pneumothorax). An immediate bedside echo is required. Once tamponade is confirmed, emergent pericardiocentesis is life-saving. Ketamine is chosen for sedation to preserve sympathetic drive and avoid further cardiovascular collapse. An apical approach is selected for the needle to minimize distance to the fluid collection under direct ultrasound visualization.
Diagnostics & Findings
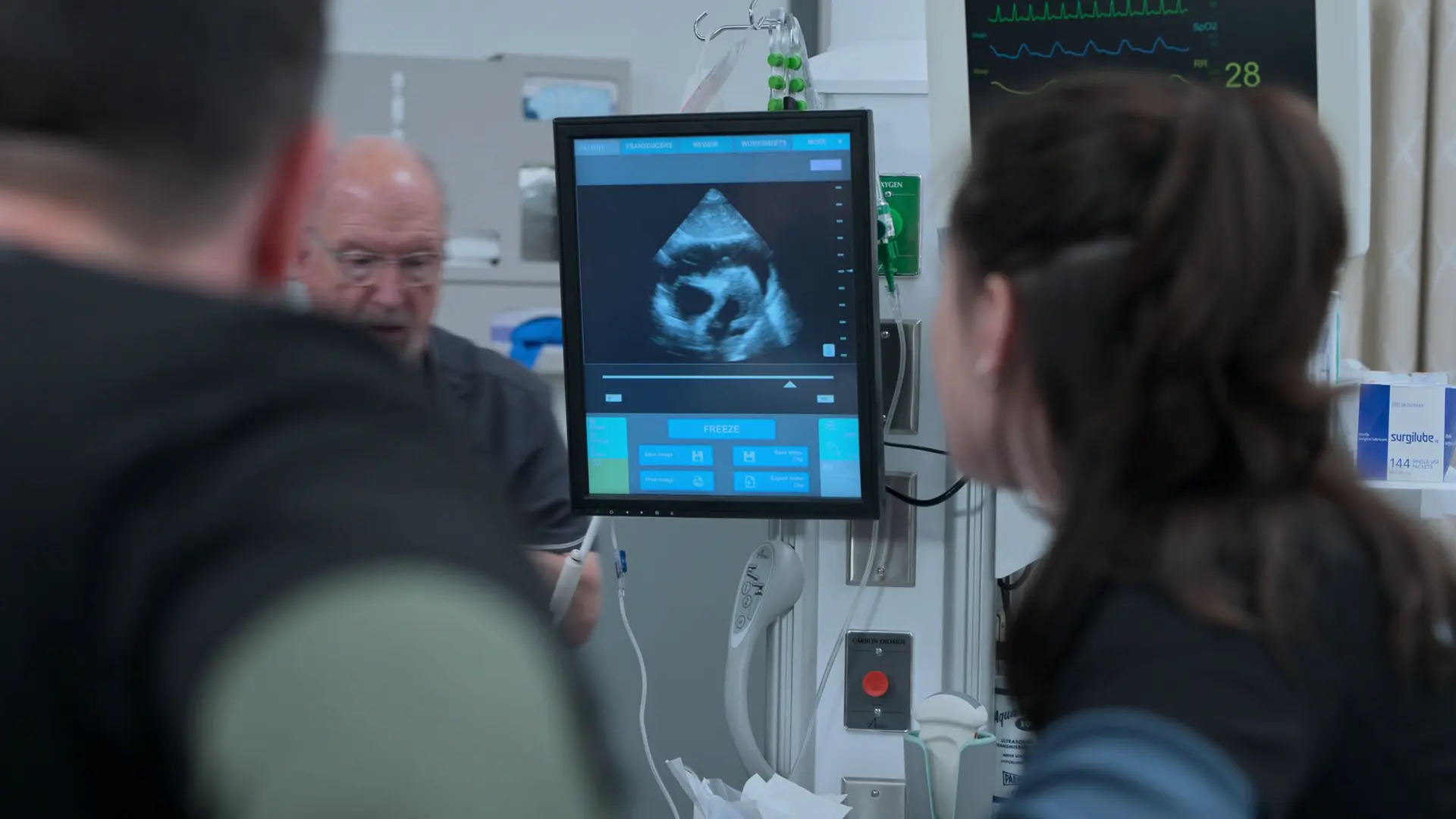
- Bedside Echocardiogram
Findings:
- Jugular Venous Distension (JVD)
- Pericardial effusion with Right Ventricular (RV) diastolic collapse
- Systolic BP dropped to 64 mmHg
Interventions
- 500cc IV fluid bolus
- 100% O2 via Non-Rebreather mask
- 0.5 mg/kg Ketamine IV for procedural sedation
- Ultrasound-guided pericardiocentesis (apical approach)
- Placement of J-wire and indwelling pericardial catheter with 3-way stopcock
⮑ Outcome & Reassessment
Removal of 40cc of blood resulted in immediate hemodynamic improvement. Systolic BP rose to 90 mmHg, and carotid pulse strengthened. Patient stabilized for transport to the OR.
Clinical Media


Diagnoses & Disposition
Evolving Diagnoses
- [Trauma Bay]Deep Scalp Laceration
- [Post-CT Review]Isolated Sternal Fracture
- [Crash Assessment]Cardiac Tamponade secondary to traumatic Right Atrial tear
Current Disposition
Admitted to Operating Room (Cardiothoracic Surgery) for definitive repair of right atrial tear.
Casebook Analysis
Episode Context
Dante serves as the high-stakes, end-of-shift 'crash' patient. His sudden deterioration delays Dr. Robby from leaving the hospital on time and provides a high-stress teaching moment for Trinity Santos, who successfully performs an apical pericardiocentesis under pressure.
Attending's Review
Medical Accuracy
The presentation of delayed cardiac tamponade from a blunt sternal fracture (causing a slow right atrial tear) is medically accurate and a known pitfall in trauma. Using Ketamine for procedural sedation in a hemodynamically unstable patient is a smart choice, as it relies on catecholamine release to support blood pressure, unlike Propofol which would cause a lethal drop. The apical approach for pericardiocentesis, while less standard than the subxiphoid approach, is acceptable and sometimes preferred when using direct ultrasound guidance if the fluid collection is closest to the apex.
Complications & Errors
- The initial assessment correctly cleared the patient based on a negative FAST and CT, but blunt cardiac injury can have delayed manifestations. The team properly decided to observe him rather than discharge him, which ultimately saved his life.
Clinical Pearls
Beck's Triad (Hypotension, JVD, and Muffled Heart Sounds) is the classic presentation for Cardiac Tamponade. In the ED, ultrasound is faster and more reliable than listening for muffled heart sounds.
A negative FAST exam on arrival does not rule out evolving hemorrhage. Serial examinations are crucial, especially in high-energy mechanisms like blast injuries.
Ketamine is the induction agent of choice in hypotensive/shocked patients requiring sedation, as it generally preserves or elevates blood pressure through sympathetic stimulation, though extreme caution must still be used in severe cardiogenic or obstructive shock where catecholamines are already maxed out.
Deep scalp lacerations that violate the galea aponeurotica will gape widely due to the antagonistic pull of the frontalis and occipitalis muscles. Suturing the galea is essential to relieve tension on the skin and allow for proper wound approximation.
A proper multi-layer closure of the scalp prevents the formation of a subgaleal hematoma. It also seals off the 'danger zone' of the scalp (the loose areolar connective tissue layer), preventing superficial infections from spreading via emissary veins into the intracranial dural venous sinuses.
Using staples for the outermost skin layer of the scalp is often preferred in the ED because it is faster than suturing, causes less damage to hair follicles, and reduces the risk of localized tissue ischemia.
In acute traumatic cardiac tamponade, the pericardial sac is stiff and does not have time to stretch. Removing even a small volume of fluid (as little as 20-50 cc) can dramatically decrease intrapericardial pressure and restore cardiac output.
When performing emergency pericardiocentesis for a suspected active bleed (e.g., atrial or ventricular tear), placing an indwelling catheter with a three-way stopcock is critical. This allows for repeated drainage of re-accumulating blood to bridge the patient to definitive surgical repair.
POCUS has revolutionized pericardiocentesis. Instead of relying solely on the traditional blind subxiphoid landmark approach, clinicians can now scan to identify the largest fluid pocket closest to the chest wall, frequently making an apical or parasternal approach safer and more direct.