History of Present Illness
Patient is an adult female with a known history of Sickle Cell Disease who was forcibly removed from a city bus and brought to the ED by EMS and police for 'disrupting and disturbing passengers.' Prehospital personnel labeled her as 'combative' and 'drug-seeking' because she was screaming for narcotics and possessed an empty Percocet bottle filled 5 days prior. Upon arrival, the patient was physically struggling with staff, stating her home medications were not working and that she was experiencing a severe vaso-occlusive sickle cell crisis.

Emergency Department Course
Triage & Acute Resuscitation
Patient arrives via EMS with police/paramedics physically restraining her, assuming she is a drug addict seeking a fix.
+1
Triage & Acute Resuscitation
Patient arrives via EMS with police/paramedics physically restraining her, assuming she is a drug addict seeking a fix.
Medical Decision Making
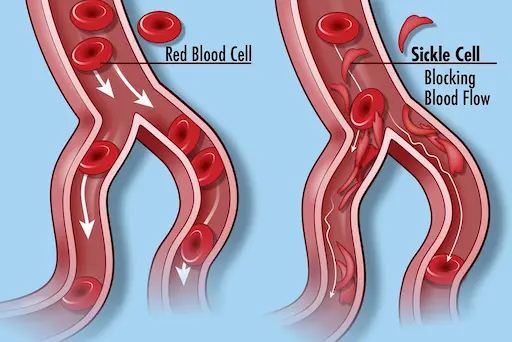
Dr. Mohan immediately recognizes the signs of a genuine vaso-occlusive crisis (VOC) and intervenes to stop the physical restraint. She understands that sickle cell pain is excruciating microvascular ischemia and that patients often have high opioid tolerances. The immediate goal is to de-escalate the psychological trauma, validate the patient's condition, and provide aggressive, rapid-onset analgesia.
Diagnostics & Findings
- Verbal confirmation of Sickle Cell history
- Stat Labs (CBC, Reticulocyte count, Type and Screen)
Findings:
- Patient is in severe pain, not merely drug-seeking.
Interventions
- Verbal de-escalation and removal of physical restraints
- 10 mg IV Morphine ordered immediately (to be repeated in 5 minutes if needed)
- Initiated an IV Dilaudid (Hydromorphone) drip
⮑ Outcome & Reassessment
Patient begins to calm down emotionally once validated and assured she is safe, awaiting the onset of the IV opioids.
Clinical Media

Reassessment & Bedside Education
Status check after 20 mg of IV Morphine has been administered.
+3
Reassessment & Bedside Education
Status check after 20 mg of IV Morphine has been administered.
Medical Decision Making
The patient is tolerating 20 mg of IV Morphine without respiratory depression, confirming a massive baseline opioid tolerance. The patient's home regimen (90 mg ER Morphine BID + PRN Oxycodone) justifies the need for high-dose continuous ED management. Labs returned showing a Hemoglobin of 6 g/dL. Given the severe anemia and intractable pain, an exchange transfusion is indicated to physically remove sickled red blood cells and replace them with healthy donor cells, improving oxygen carrying capacity and halting the crisis. Dr. Mohan uses this moment to correct her junior colleague's implicit bias regarding the 'surprising' opioid dosage.
Diagnostics & Findings
- CBC Results Review
Findings:
- Hemoglobin critically low at 6 g/dL
- Patient's home opioid regimen is exceptionally high, confirming tolerance
Interventions
- Ordered an Exchange Transfusion
- Started continuous IV Dilaudid (Hydromorphone) at 4 mg/hr via PCA (Patient-Controlled Analgesia)
⮑ Outcome & Reassessment
Pain is reported as 'a little better'. Patient anticipates and agrees with the plan for an exchange transfusion.
Clinical Media

Family Update & Apology
Patient's wife, Ondine, arrives at the bedside.
Family Update & Apology
Patient's wife, Ondine, arrives at the bedside.
Medical Decision Making
With the acute medical crisis stabilized by continuous Dilaudid and an impending exchange transfusion, the physician's focus shifts to patient advocacy, psychological first aid, and repairing the hospital-patient relationship after the initial biased trauma inflicted by EMS/Triage.
Diagnostics & Findings
Findings:
- Patient is visibly relieved and states she feels 'so much better.'
Interventions
- Formal apology delivered to the patient and her wife for the implicit bias and poor treatment upon arrival
- Assurance of continued, aggressive, and respectful sickle cell crisis management
⮑ Outcome & Reassessment
Patient and family are appreciative and trust has been established with the treating physician.
Diagnoses & Disposition
Evolving Diagnoses
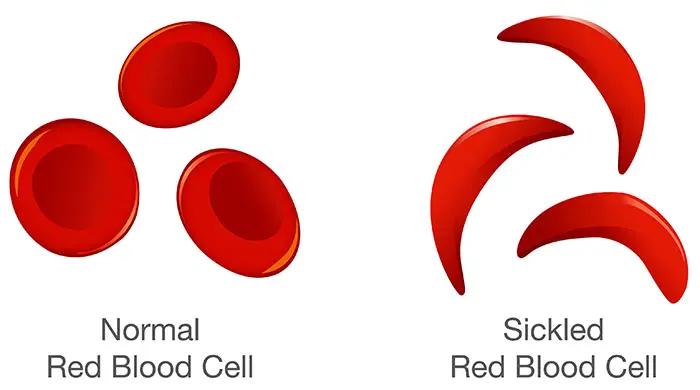
- [S01E02]Vaso-occlusive Crisis (VOC) secondary to Sickle Cell Disease
- [S01E02]Severe Anemia (Hemoglobin 6 g/dL)
Current Disposition
Admitted for Exchange Transfusion and continuous IV Pain Management.
Casebook Analysis
Episode Context
The case serves as a powerful narrative on implicit bias and racial disparities in healthcare. It highlights the frequent mistreatment of Sickle Cell patients, who are overwhelmingly Black and are often wrongfully labeled as 'drug-seeking' or 'addicts' due to their chronic pain conditions and correspondingly high opioid tolerances.
Attending's Review
Medical Accuracy
The medical depiction is highly accurate and socially poignant. Sickle Cell patients often require massive doses of opioids during a VOC to overcome their baseline tolerance (e.g., this patient's home regimen of 90mg ER Morphine BID + PRN Oxycodone). The doses administered in the ED (10-20mg IV Morphine followed by a 4mg/hr Dilaudid drip) would cause fatal respiratory depression in an opioid-naive patient, but are realistic and necessary for a tolerant patient in severe crisis. The description of the pain as 'electrical stabbing' and 'flushing glass' accurately reflects the microvascular ischemia typical of the disease. Furthermore, ordering an exchange transfusion for a hemoglobin of 6 in the setting of severe, refractory VOC is an appropriate and aggressive standard of care.
Complications & Errors
- Prehospital Implicit Bias: EMS and police assumed the patient was a drug addict acting out on a bus, physically restraining her and escalating her physiological and psychological stress. They completely missed a life-threatening hematologic crisis based on preconceived prejudices regarding her behavior and an empty prescription bottle.
Clinical Pearls
Sickle Cell Vaso-Occlusive Crisis (VOC) causes extreme ischemic pain. Standard ED opioid protocols often severely under-dose these patients; always ascertain and account for their baseline home opioid tolerance.
Beware of implicit bias: Chronic pain patients, especially minorities with Sickle Cell Disease, are disproportionately labeled as 'drug-seeking'. Validate their pain, check their objective markers (like a Hemoglobin of 6), and treat aggressively.
Exchange transfusions may be indicated in severe sickle cell complications (e.g., Acute Chest Syndrome, stroke, or severe refractory VOC with profound anemia) to physically remove the sickled erythrocytes and replace them with normal hemoglobin.


