History of Present Illness
78-year-old female presents to the ED after her husband's car backed into her at a very low speed, causing a ground-level fall. She denies head trauma, chest pain, or shortness of breath. She complains of left hip pain and has visible bruising. Past medical history is significant for hypertension, hypothyroidism, and atrial fibrillation. She is currently anticoagulated on Eliquis (apixaban).

Emergency Department Course
Triage & Initial Evaluation
Patient arrives in the ED after an auto vs. pedestrian accident.
+3
Triage & Initial Evaluation
Patient arrives in the ED after an auto vs. pedestrian accident.
Medical Decision Making
Patient sustained a ground-level fall with direct impact to the left hip. The lack of leg shortening or external rotation reduces the clinical suspicion for a major displaced femur or hip fracture, but a fracture cannot be ruled out clinically. More concerning is her use of Eliquis (apixaban), which significantly increases the risk of occult internal bleeding or retroperitoneal hematoma. A CT of the Abdomen/Pelvis is indicated over a plain film X-ray to concurrently evaluate for a subtle pelvic ring fracture and internal hemorrhage.
Diagnostics & Findings
- Physical Examination
- CT Abdomen/Pelvis ordered
- Laboratory studies ordered
Findings:
- Large bruise on left hip
- Tenderness to palpation over the left hip
- No leg shortening or external rotation observed
Interventions
- Morphine 4mg IV
- Zofran IV (to prevent opiate-induced nausea)
⮑ Outcome & Reassessment
Patient tolerates the initial exam well and awaits imaging.
Clinical Media



Family Discussion & Caregiver Assessment
Patient's daughter arrives seeking an update; physician identifies an unsafe discharge environment.
Family Discussion & Caregiver Assessment
Patient's daughter arrives seeking an update; physician identifies an unsafe discharge environment.
Medical Decision Making
Geriatric emergency medicine requires treating the patient's psychosocial environment. The patient's husband, Eddie, exhibits a broad-based, unsteady gait and failed an informal Romberg test. If Frida has a hip injury requiring mobility assistance, Eddie will be physically unable to provide it, resulting in an 'unsafe to return home' disposition. The physician begins laying the groundwork for temporary assisted living or inpatient rehabilitation.
Diagnostics & Findings
- Informal functional assessment of the primary caregiver (husband)
Findings:
- Husband exhibits unsteady gait and balance issues.
Interventions
- Discussion of assisted living and rehabilitation options with the daughter and husband.
⮑ Outcome & Reassessment
Husband is resistant to the idea of assisted living, increasing the complexity of the eventual discharge.
Imaging Review & Disposition Planning
CT Abdomen/Pelvis results are returned.
+1
Imaging Review & Disposition Planning
CT Abdomen/Pelvis results are returned.
Medical Decision Making
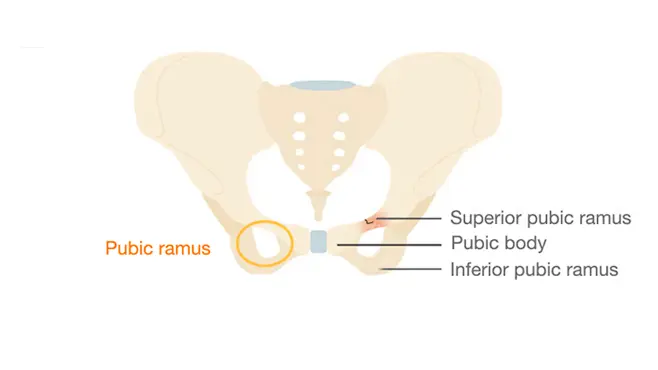
The CT scan ruled out internal bleeding (crucial for a patient on Eliquis) and ruled out a major hip fracture. It identified a hairline fracture of the superior pubic ramus. This is a stable pelvic fracture that does not require surgical intervention. It can be managed conservatively with pain control and mobility assistance (walker). The primary hurdle is now ensuring the patient has adequate help at home, given her husband's physical limitations.
Diagnostics & Findings
- Review of CT Abdomen/Pelvis
Findings:
- Hairline fracture of the superior pubic ramus.
- No hip fracture.
- No internal hemorrhage.
Interventions
- Prescription for a walker
- Scheduling for physical therapy
- Recommendation for 6-8 weeks of limited weight-bearing/rest
⮑ Outcome & Reassessment
Patient is relieved by the diagnosis but the family remains in conflict over how to manage care at home. Dr. Mohan requests the husband's medication list to investigate his physical decline.
Clinical Media
Caregiver Medication Review
Evaluating the husband's medication list to resolve the disposition roadblock.
Caregiver Medication Review
Evaluating the husband's medication list to resolve the disposition roadblock.
Medical Decision Making
The husband is taking Meclizine (for vertigo), Methocarbamol (muscle relaxant), and Metoclopramide (gastric motility). These are all on the Beers Criteria list of potentially inappropriate medications for older adults. The cumulative anticholinergic burden is likely causing his drowsiness, balance issues, and unsteady gait. Adjusting these medications via his PCP could restore his functionality, thereby making the home environment safer for the patient.
Diagnostics & Findings
- Medication reconciliation for the caregiver
Findings:
- Identification of multiple anticholinergic/sedating medications impacting the caregiver's mobility.
Interventions
⮑ Outcome & Reassessment
Plan formulated to discharge the patient home with robust support, avoiding the need for a forced placement in a nursing facility.
Final Discharge Planning
Finalizing the disposition plan with the patient and family.
Final Discharge Planning
Finalizing the disposition plan with the patient and family.
Medical Decision Making
By organizing an aggressive outpatient support system (Medicare-funded home health nurse, physical therapy, and community support like personal shoppers) and addressing the husband's reversible pharmaceutical impairments, the medical team successfully preserves the patient's autonomy while ensuring clinical safety.
Diagnostics & Findings
Interventions
- Arranged home physical therapy
- Arranged visiting home nurse
- Care management integration (Area Agency on Aging)
- Advice to follow up with husband's PCP to deprescribe inappropriate medications
⮑ Outcome & Reassessment
The family accepts the home-care plan and agrees to tour an assisted living facility as a backup, resolving the disposition conflict.
Diagnoses & Disposition
Evolving Diagnoses
- [Triage & Initial Evaluation]Left hip contusion; Rule out occult hemorrhage; Rule out pelvic/hip fracture
- [Imaging Review & Disposition Planning]Hairline fracture of the superior pubic ramus
Current Disposition
Discharged to home. Management includes a walker, at-home physical therapy, visiting nursing support, and a recommendation for the patient's husband to undergo medication deprescribing with his PCP to improve his capability as a caregiver.
Casebook Analysis
Episode Context
Frida's case serves as a poignant exploration of Geriatric Emergency Medicine and Social Medicine. It highlights that emergency physicians must often treat the entire family unit, as the safety of an elderly patient's disposition is directly tied to the health and capabilities of their primary caregiver.
Attending's Review
Medical Accuracy
Highly accurate. The decision to bypass a plain X-ray and go straight to a CT Abdomen/Pelvis is standard of care for an elderly patient on a direct oral anticoagulant (Eliquis) following blunt trauma, as occult retroperitoneal bleeding is a major risk. Furthermore, the identification of Meclizine, Methocarbamol, and Metoclopramide as culprits for the husband's gait instability is an excellent, realistic application of the AGS Beers Criteria for Potentially Inappropriate Medication Use in Older Adults.
Clinical Pearls
In elderly patients on systemic anticoagulation (e.g., apixaban, rivaroxaban, warfarin), a ground-level fall warrants a low threshold for advanced imaging (CT) to rule out life-threatening occult bleeds, even if the trauma appears minor.
A superior pubic ramus fracture is one of the most common pelvic fragility fractures. It is typically mechanically stable and can be managed conservatively with pain control and progressive weight-bearing.
A safe ED discharge requires assessing caregiver capacity. Polypharmacy and anticholinergic burden (often identifiable via the Beers Criteria) are frequent, reversible causes of falls and functional decline in older adults.